

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ruptured vertebral artery dissecting aneurysms (VADAs) presented with acute subarachnoid hemorrhage (SAH) have a high incidence of rebleeding and mortality rate compared with saccular aneurysms [1, 2]. Immediate treatment with surgical or endovascular approach is necessary to prevent devastating rebleeding [3]. Surgical clipping of VADAs has several limitations because of deep location of aneurysms and their close relationship to lower brain stem and lower cranial nerves [4].
Unruptured VADAs may present with severe occipital headache or focal neurologic def icits due to vertebrobasilar ischemia without aggressive clinical course. The optimal treatment of unruptured VADA is still unknown [3, 5]. As the reported risk of bleeding from unruptured VADA in recent studies is higher than those in the previous reports, endovascular treatment should be considered in cases which have unfavorable angiographic features [1, 6].
Follow-up imaging findings of untreated VADAs, such as gradual disappearance of the luminal narrowing or progressive enlargement of the aneurysmal dilatation, have been reported [7, 8]. However, the results of serial angiographic follow-up combined with clinical outcomes after endovascular treatment especially with stent-assisted coiling have been rarely reported. Thus, the purpose of this study was to report immediate and follow-up angiographic results and clinical outcomes in 45 VADAs, which were managed with various endovascular techniques.
MATERIALS AND METHODS
Patients
Institutional Review Board approval was obtained, with informed consent being waived. From July 2002 to September 2013, a total of 42 patients having 45 VADAs were treated with endovascular treatment at single institution. The study group consisted of 23 males and 19 females (mean age, 52 years; age range, 36 to 80 years). Of the 45 VADAs, 17 were ruptured aneurysms and 28 were unruptured.
Endovascular Treatment
Decision of endovascular treatment method was based on the angiographic characteristics of VADAs, presence or absence of SAH, and clinical presentations. Internal trapping by detachable coils was primarily considered when the VADA was located in proximal or distal to origin site of PICA. Stent implantation or stent-assisted coil embolization was considered in cases of unruptured aneurysms with posteroinferior cerebellar artery (PICA) involvement. As a result, various endovascular strategies were used: internal trapping with coils (n=26), stent-assisted coil embolization (n=14), and stent implantation only (n=5).
Imaging Analysis
MRI and angiographic findings were evaluated by single interventional neuroradiologist. The diagnosis of VADA was based on the characteristic appearances revealed on MRA, computed tomography angiography (CTA) or conventional angiography. VADA was located in right vertebral artery in 28 cases and in left vertebral artery in 17 cases. Involved vertebral artery was dominant artery in 10 cases and non-dominant in 19 cases. No vertebral artery dominance in 16 cases. 19 VADAs were located distal to the origin of PICA, 18 VADAs were proximal to that of PICA, and 8 VADAs were PICA involvement type. Immediate angiographic results were classified as complete or incomplete occlusion based on the completion angiography. Follow-up angiographic results were evaluated with CTA, MRA, or DSA more than 3 months later. These results were classified as complete occlusion, antegrade recanalization, no change, complete occlusion with vessel remodeling, and recanalization.
Analysis of the clinical results
The clinical data was reviewed retrospectively by a neurologist using the Hunt and Hess grading system (H&H grade) and modified Rankin Scale (mRS) at 3-months. Clinical outcomes were assessed at 3months after endovascular treatment. In patients with unruptured VADA, favorable outcome was defined as mRS 0 and 1.
RESULTS
Ruptured vertebral artery dissecting aneurysm
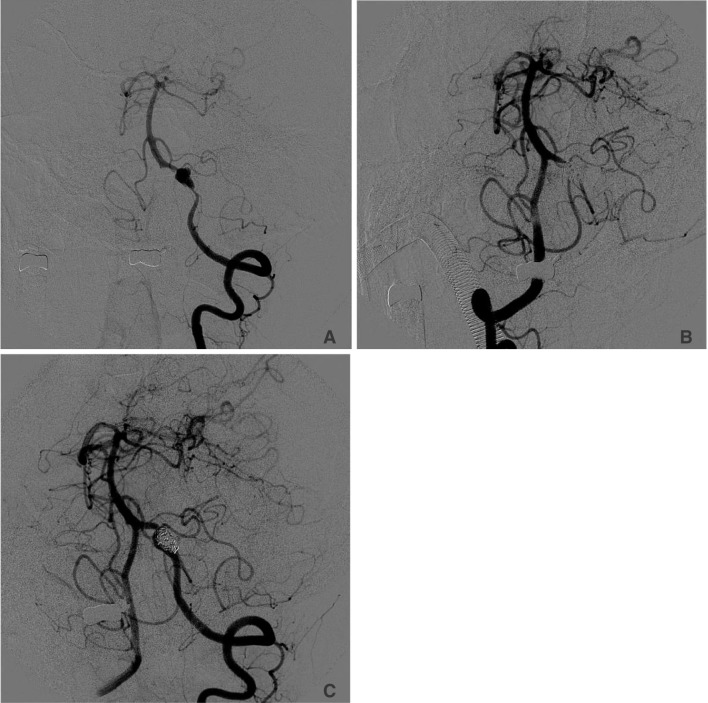
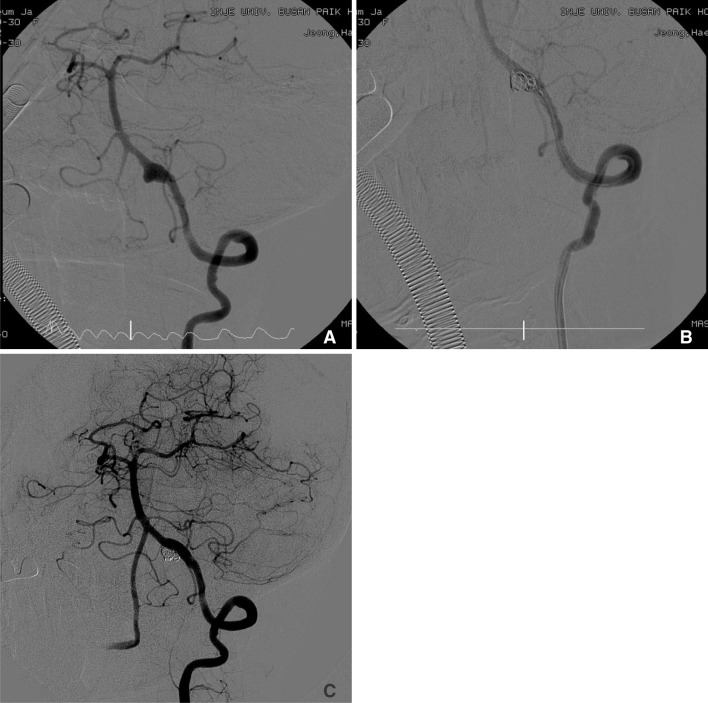
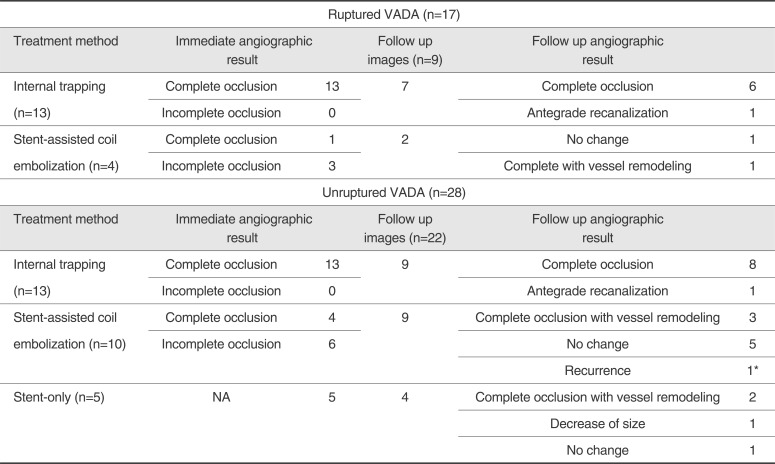
Of 17 ruptured VADAs, 5 cases initially presented with poor grades (4 or 5), 8 cases with grade 3, 2 cases with grade 2, and 1 patient with grade 1. Results of immediate and follow up imaging studies in ruptured VADAs are presented in the table. In ruptured cases (n=17), endovascular treatment consisted of internal trapping with coil embolization (n=13) and stent-assisted coil embolization using self-expandable stent (n=4). Immediate angiographic results revealed complete occlusion in 14 cases and incomplete occlusion in 3 cases. Eight cases were lost to follow up. Follow up imaging study in 7 cases treated with internal trapping revealed complete occlusion in 6 cases and antegrade recanalization in 1 case (Fig. 1). In 2 cases treated with stent-assisted coil embolization, follow up imaging studies showed no change in 1 case and complete occlusion with vessel remodeling in 1 case (Fig. 2). There were 6 procedure-related complications: lateral medullary infarction (n=2), embolic infarction (n=2), unintended arterial occlusion (n=1), and parent artery dissection (n=1). Follow-up mRS was available in 13 patients. Favorable outcome (mRS 0 and 1) was achieved in 5 patients and poor outcome in 8 patients. Four patients died.
Unruptured vertebral artery dissecting aneurysm
Of 28 unruptured VADAs, 25 VADAs initially presented with headache, 2 with hemiparesis, and 1 with lateral medullary infarction. Results of immediate and follow-up imaging studies in unruptured VADAs are presented in table. In unruptured cases, internal trapping was performed in 13 cases, stent-assisted coil embolization in 10 cases, and stent implantation only in 5 cases. All VADAs treated with internal trapping showed complete occlusion on immediate post-procedural angiography. Immediate angiographic results in 10 cases treated with stent-assisted coliling showed complete occlusion in 4 cases and incomplete occlusion in 6 cases. Stent implantation was successful in all 5 cases treated with stenting only.
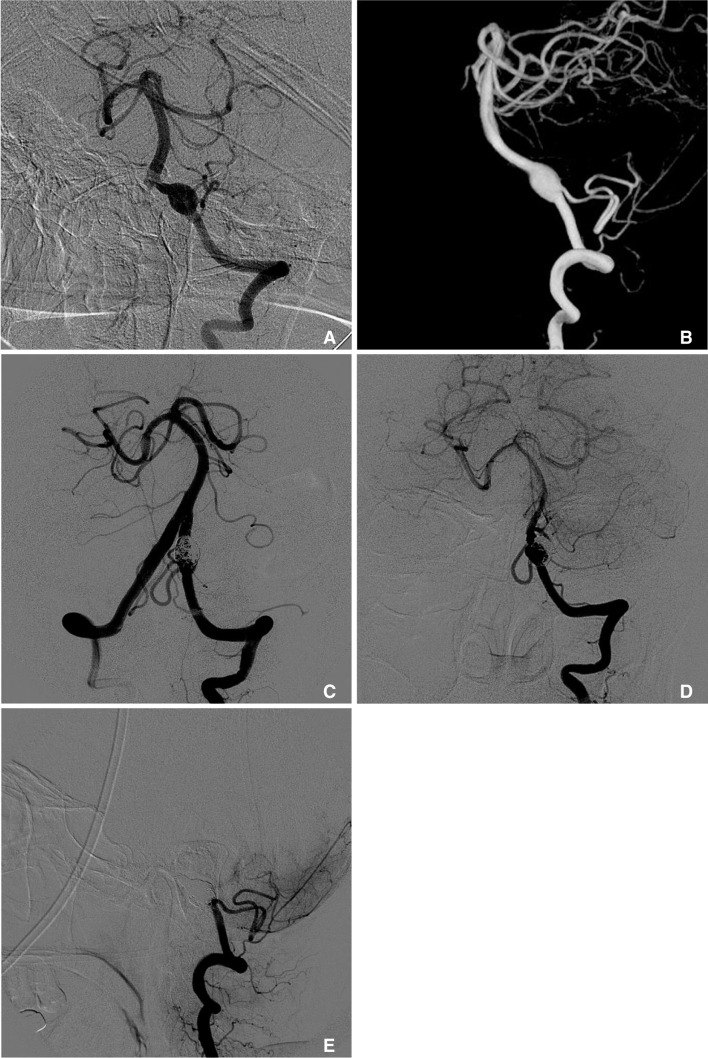
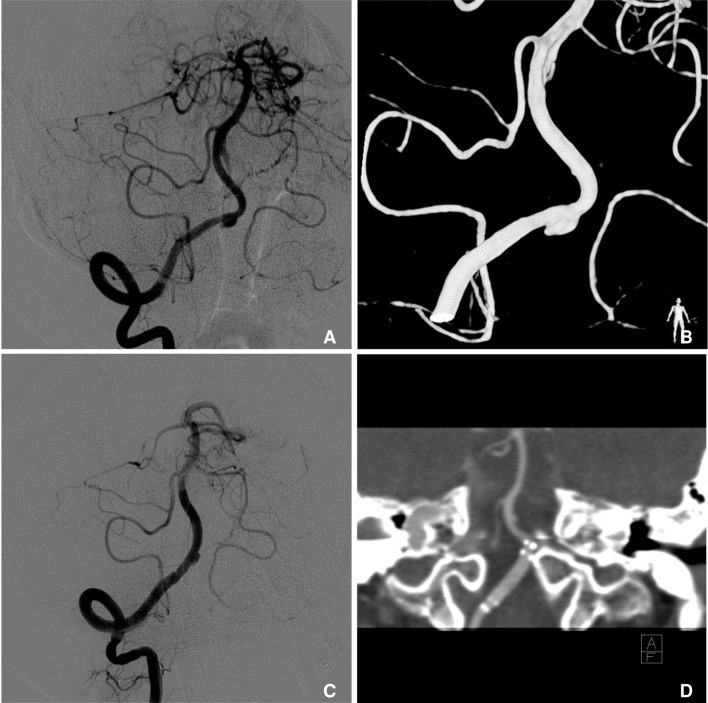
Follow-up angiographic studies were available in 22 cases. In 9 cases treated with internal trapping, complete occlusion occurred in 8 cases and antegrade recanalization in 1 case. In 9 cases treated with stent-assisted coil embolization, complete occlusion with vessel remodeling occurred in 3 cases, no change in 5 cases, and recanalization in 1 case. Of these, a patient with recanalization on follow-up after stent-assisted coil embolization underwent retreatment with internal trapping using detachable coils (Fig.3). In cases treated with stenting only, complete occlusion with vessel remodeling occurred in 2 cases (Fig. 4), decrease of sac in size in 1 case, and no change in 1 case.
Follow-up mRS was available in all patients. Favorable outcome (mRS 0-1) was achieved in 26 cases and poor outcome (mRS 2-5) in 2 cases. There was no mortality. There was one case of lateral medullary infarction as a post-procedural complication.
DISCUSSION
Primary mechanism of the arterial dissection is disruption of the internal elastic lamina. After disruption, leukocyte and macrophage infiltration, endothelial coverage, and neointima formation follow subsequently [3]. SAH occurs due to rupture of the thin layer of intradural adventitia [9]. Ruptured VADA shows high incidence (over 70%) of rebleeding within 24 hours which results in poor clinical outcome [3, 9, 10]. Endovascular intervention is mandatory to prevent these fatal rebleeding. Two main concepts in the endovascular treatment of the VADA are deconstructive and reconstructive techniques for the parent vessels. First, deconstructive techniques can be performed by balloon or coil embolization [11, 12, 13, 14, 15, 16]. Multiple studies regarding direct occlusion of the pathologic segment were reported [17, 18]. However, there were several case reports of antegrade recanalization after endovascular treatment for ruptured VADAs [19, 20]. The mechanism of the antegrade recanalization can be explained as following [10]; (1) if microcatheter navigate into the false lumen and occlude the false lumen with detachable coils, true lumen dilates into the normal diameter as false lumen collapses (2). Detachable coils were insufficient to cover the entry of the dissecting aneurysm. In our case, there was one ruptured VADA case which showed antegrade recanalization 6 months after internal trapping (Fig. 1).
Especially in case of VADA involving PICA in dominant side, alternative technique such as proximal occlusion can be considered. However, proximal occlusion technique can cause retrograde flow from the contralateral vertebral artery resulting in rebleeding [14]. In our study, although there were 8 cases of VADAs involving PICAs, none of those was treated in proximal occlusion technique.
Reconstructive techniques were applied to VADAs with stenting or stent-assisted coiling. Canton et al. [21] and Lopes et al. [22] reported the mechanism of endovascular stent deployment in VADA. They suggested flexible stents reduces the stresses acting on the aneurysm wall which results in true lumen expansion and parent artery reconstruction finally. Histologically, complete endothelialization of the stent and fibroelastic tissue formation along the aneurysmal neck explain mechanism of the stent deployment strategy. In recent reports, outcome of endovascular treatment with stenting in ruptured or unruptured VADA is favorable [1].
Although unruptured VADAs usually show benign clinical course, the natural course of the unruptured VADAs is still unknown and treatment guideline remains controversial. Administration of antiplatelet or anticoagulant in patients with unruptured VADAs and ischemic presentations may exacerbate aneurysmal dissection and cause rupture of the aneurysm. Risk of bleeding from unruptured VADA was higher than previous reports and endovascular treatment should be considered in some cases, such as in cases of increased size of aneurysmal dilatation during follow-up period and when double lumen sign is visible in the acute stage[6]. For making a decision of parent artery occlusion in cases of unruptured VADA, there are several factors to be considered: risk of bleeding in conservative treatment; risk of ischemic complications during procedure; blood supply from the anterior and posterior spinal artery, perforating arteries, and patency of contralateral vertebral artery; and relationship between aneurysm and PICA [3]. Reconstructive techniques, stent placement with or without coil embolization, aims at the preservation of the vertebral artery flow. This technique, as well as parent artery occlusion, show favorable results in unruptured VADA cases according to several reports [4, 23]. In our study, clinical and radiologic results were satisfactory in upruptured patients treated with internal trapping and stent placement with or without coils. Only one case revealed recanalization of the dissecting aneurysm after 1 year, which was retreated with internal trapping (Fig. 3). In one case, there was lateral medullary infarction 2 days after internal trapping. Although PICA has rich pial anastomoses, there have been case reports of PICA infarction on follow up images after endovascular procedure [3]. They suggested that thromboembolism due to coil loop herniation into the PICA origin and occlusion of a perforating artery was possible causes of the PICA territory infarction. However, as well as procedural complication, recurrent ischemia in unruptured VADA patients may be attributable to thrombotic occlusion of the stenotic lesion, distal emboli, to further occlusion of perforating arteries originating from the VA due to progression of the dissection.
The major limitations of our study were the small number of cases and the retrospective nature of the study.
 XML Download
XML Download