

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The Neuroform EZ Stent System (Boston Scientific Corporation, Fremont, CA, USA) is a fourth generation intracranial aneurysm stent system approved for use in the US by the Food and Drug Administration to treat wide-neck aneurysms in conjunction with endovascular coiling [1]. Predicated on the technology of early generation stent systems, there have been structural and mechanical modifications to the Neuroform EZ Stent System (NF-EZ) to facilitate positioning, deployment, and vascular accessibility. The NF-EZ Directions for Use (DFU) outlines a standard technical approach and discourages physical tampering of the stent system. In this technical note, the standard stent deployment was impeded as a result of the newly integrated preshaped distal guidewire. To overcome this, the NF-EZ guidewire was removed using surgical scissors. Successful stent implantation and aneurysm coiling were consequently achieved.
TECHNICAL CASE REPORT
An adult male was discovered unconscious at home and a CT head demonstrated diffuse subarachnoid hemorrhage, mild ventricular hemorrhage and hydrocephalus. On subsequent CT angiogram of head, a moderately wide neck 3 mm left anterior communicating artery (ACom) aneurysm was identified. The patient was taken to the neurointerventional suite, where the small ACom aneurysm was successfully coiled (Axium, Covidien Corporation, Plymouth, MN, USA). On 6-month follow-up MR angiogram of the head, a small recurrent aneurysm was discovered, so a stage-II embosurgery was scheduled.
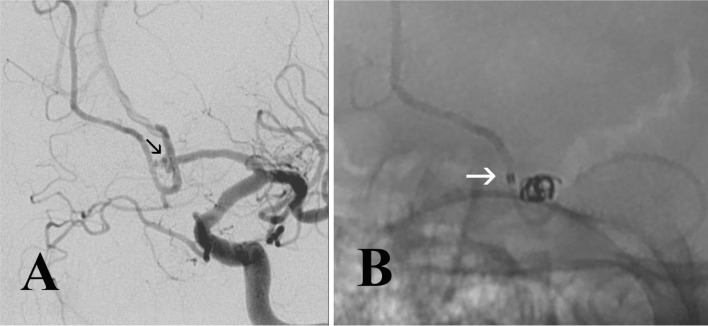
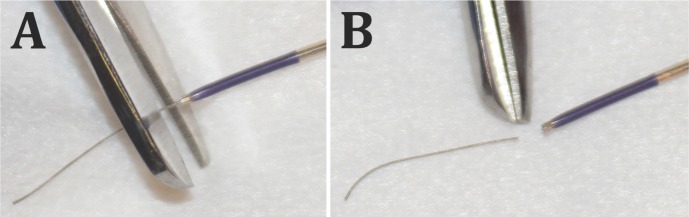
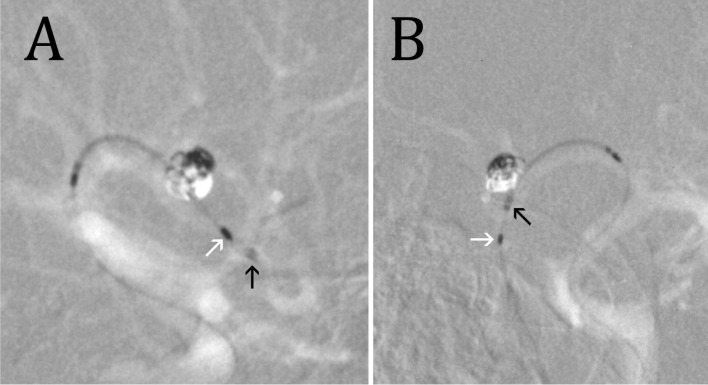
The patient was pre-operatively medicated with aspirin and clopidogrel. Under general anesthesia, a 6-French right femoral artery sheath was placed. Intravenous heparin and 1 g of cefazolin were administered. A 6-French guidecatheter was placed in the left ICA. Using multiple microcatheters and microwires in varying combinations, the intracranial circulation was explored. The recurrent aneurysm was noted to be small, measuring about 2 mm, and which demonstrated a wide base that incorporated portions of the left ACom and the left A2 (Fig. 1A). Given this configuration plus the associated tortuous vascularity, stent-assisted coiling was elected. A Marksman catheter (Covidien Corporation) was primarily advanced over numerous microwires in an unsuccessful attempt to gain access in the left A2 distal to the aneurysm. As a result, exchange wire technique was used: An SL-10 microcatheter (Boston Scientific Corporation, Fremont, CA, USA), was successfully advanced over exchange length Synchro2 microwire (Boston Scientif ic Corporation). With the wire at the left A2-3 junction, the SL-10 microcatheter was withdrawn. Over this exchange wire, the Marksman catheter was advanced as far as possible into the left A2, that is, approximately 1 cm beyond the aneurysm (Fig. 1B). Advancing this catheter any further was prevented by a combination of the general vascular tortuosity and the relatively small caliber of the A2. A 2.5 × 15 mm NF-EZ stent was brought to the field, prepped, and advanced through the Marksman catheter. Though the NF-EZ stent system advanced easily, the Marksman catheter slightly retreated with its tip adjacent to the most proximal A3 subfrontal branch. The NF-EZ guidewire readily entered this small vessel instead of continuing around into the distal A2. An attempt to advance the stent with the wire in this small branch was met with additional resistance and threatened further retreat of the Marksman catheter. Because of the added length of the NF-EZ guidewire, the stent apparatus could not be positioned completely across the aneurysm orifice, and so it was withdrawn. The stent apparatus was examined and found to be free of defect or otherwise adversely affected by the attempt to place it. But to gain sufficient intracranial purchase of the stent, the guidewire was snipped off flush using surgical scissors at the junction with the distal stent bumper (Fig. 2). The stent was readvanced into the Marksman catheter and easily placed across the aneurysm neck. With the distal guidewire now removed, care was taken to ensure that forward motion of the stent delivery system did not advance beyond the tip of the Marksman catheter. With the stent positioned across the aneurysm, the Marksman catheter was manually withdrawn, unsheathing the stent in an acceptable position-- completely crossing the aneurysm orifice, extending from the left A2 into the left A1 (Fig. 3). The stent delivery system was then removed without disturbing the stent. Aneurysm coiling proceeded uneventfully at that point (Deltapaq and Deltaplush, Codman & Shurtleff Inc, Raynham, MA, USA). Final angiography demonstrated an adequately packed aneurysm with coils completely secured in the aneurysm by the stent (Fig. 4). The patient did well post-operatively, and remains neurologically intact, functionally independent and fully employed (most recent follow-up at 15 months). Because the above NF-EZ modification represented a device protocol deviation, it was reported to both the local IRB and the device's sponsor in a timely fashion.
DISCUSSION
The NF-EZ is the latest offering from the Neuroform stent family. Like its predecessors, the NF-EZ stent renders mechanical and hemodynamic benefits for aneurysm repair by preventing and repairing coil protrusion into the parent artery, reducing intra-aneurysmal flow, and promoting aneurysm occlusion [2-4]. The NF-EZ confers several advantages over the existing third generation Neuroform Stent Delivery System. Some of the technical difficulties described with the third generation version included the en bloc advancement or transfer to a pre-positioned alternate microcatheter, which can also be time consuming and technically challenging for a single operator.
Complications can arise in conjunction with stent implantation including stent migration, maldeployment and stent herniation into the aneurysm [5, 6]. However, the NF-EZ allows the sole surgeon to more easily place the stent without the challenges of handling a long stent transfer system. Also, the addition of distal and proximal radioopaque positioning bumpers and a preshaped distal tip have, overall, facilitated precise positioning prior to, and during deployment.
In regards to this unique device modification, the standard stent pre-deployment technique failed because of mechanical impendence from the preshaped distal tip entering a small vessel branch. Friction generated from the patient's intra- and extracranial vascular tortuosity further limited the amount of forward pressure that could be placed upon the delivery and guide catheters without causing these catheters to retreat. A larger caliber or stiffer guide catheter might have obviated the need to modify the stent. Also, a third, intermediate catheter (e.g., Navien, Covidien Corporation) would potentially have offered a more robust tri-axial support system.
The Wingspan stent (Stryker, Kalamazoo, MI, USA) was considered as a back-up option if the rigid nose-cone of this stent was likewise severed as previously reported by Lesley et al [7]. But owing to the Wingspan's stent inherently greater stiffness compared to the Neuroform stent, the off-label choice of this stent was avoided. Other intracranial stents (Solitiare, Covidien Corporation; and, Enterprise, DePuY/Codman & Shurtleff, Inc, Raynham, MA, USA) as well as the Navien catheter were not stocked in-house at the time of the procedure and were therefore not considered in this case.
Any perceived benefit must be weighed against the potential for patient harm when modifying any surgical device. Before introducing the altered stent, the guide wire and distal stent bumper were meticulously scrutinized. The surgical scissors had cleanly amputated the wire from the stent, leaving no wire remnant or jagged edge. The modified stent advanced readily to the tip of the microcatheter with no tactile sensation of resistance and no fluoroscopic evidence of unexpected device function. Because of the blunt nature of the distal stent bumper, extreme care was used in the absence of the stent guide wire to ensure that the bumper did not advance unprotected within the vessel during the microcatheter unsheathing of the stent.
The NF-EZ is overall, an improved iteration compared to its predecessors. However, the preshaped distal guidewire can, on occasion, impede sufficient distal placement of the stent. Snipping off the distal guidewire may be safely performed to overcome this obstacle.

 XML Download
XML Download