

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Atherosclerotic occlusive disease of the extracranial vertebral artery (VA) is a major cause of stroke and transient ischemic attack (TIA) of the posterior circulation. Atherosclerosis commonly affects the origin and proximal portion of the VA [1], and approximately one third of patients with extracranial VA stenosis are noted to have bilateral disease [2, 3]. Occlusion or severe stenosis of the bilateral VA may cause vertebrobasilar insufficiency. Even so, there are unexpectedly only a few reports describing stroke due to an acute VA origin occlusion successfully treated endovascularily [4, 5].
The authors report a case of stroke owing to an acute occlusion of VA origin associated with contralateral hypoplastic VA leading to basilar artery (BA) thrombosis, which was treated by angioplasty with stenting and intracranial fibrinolysis.
CASE REPORT
Clinical Presentation
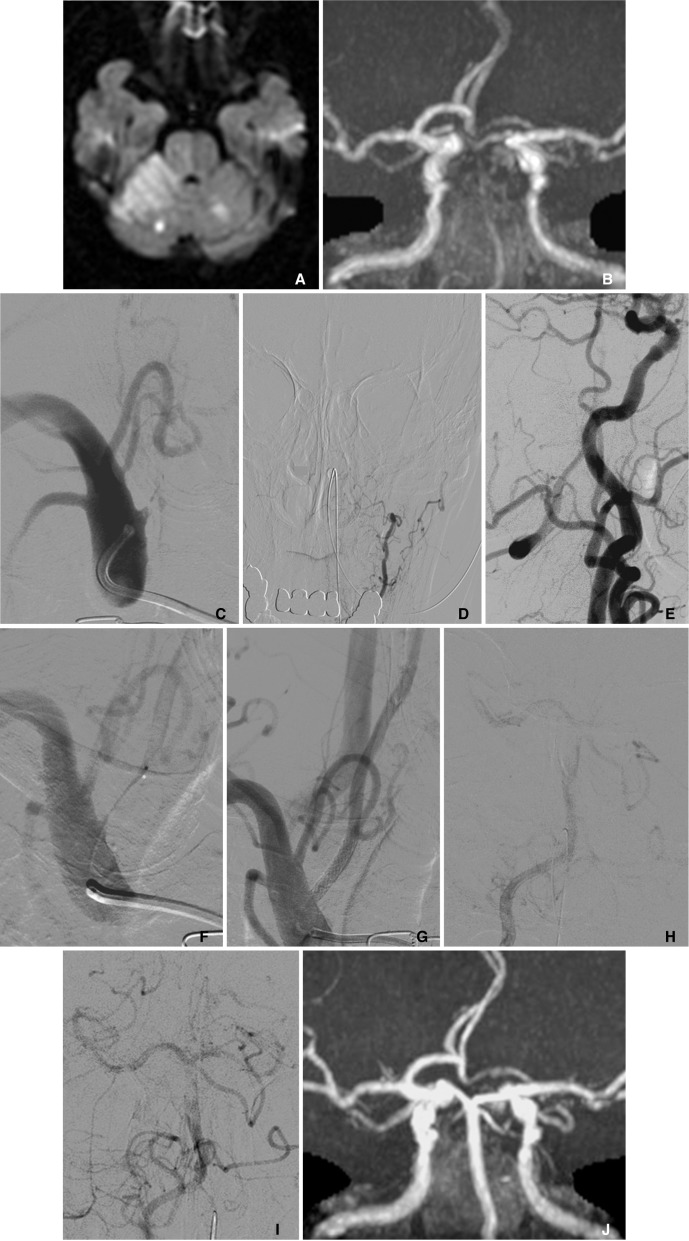
A 78-year-old man had a history of hypertension and coronary artery bypass graft for angina pectoris. However, he was not on any antiplatelet/anticoagulant medication. He was discovered after having fallen down on the street and was transferred to the hospital. He presented consciousness disturbance, left hemiparesis, dysarthria, and gaze palsy. The National Institutes of Health Stroke Scale (NIHSS) on admission was 18. MR diffusion weighted image (DWI) demonstrated a high-intensity area in the right cerebellum and brain stem (Fig. 1A). MR T2 weighted and fluid-attenuated inversion recovery (FLAIR) images showed subtle ischemic change. MR angiography (MRA) showed faint visualization in the distal part of BA and bilateral superior cerebellar arteries (SCA) (Fig. 1B).
Diagnostic cerebral angiography demonstrated that the right VA was occluded at its origin (Fig. 1C), and that the left VA was hypoplastic (Fig. 1D). The distal right VA after the midcervical portion was supplied with collateral flows via external carotid arteries and cervical arteries (Fig. 1E). The BA was filled with thrombus, although it was supplied by the antegrade flow from ipsilateral VA and the retrograde collateral flow from posterior communicating arteries. The right SCA was occluded at the origin. The left VA ended at the extracranial portion, while the left anterior inferior cerebellar artery (AICA) widely covered the left cerebellum.
The patient presented the discrepancy between the lesion on DWI and severe clinical symptom (DWI-clinical mismatch). A recombinant tissue plasminogen activator was not administered because the onset of symptoms was unknown and MR T2/FLAIR images suggested the possibility of progress of the time from onset. Therefore, endovascular intervention was immediately performed (130 minutes after the arrival at hospital).
Intervention
Intervention was carried out transfemorally under systemic heparinization. A 6 Fr guiding catheter (Envoy, Cordis Neurovascular, Miami, FL, USA) was advanced to the right subclavian artery. Penetration of the occlusive site proved too difficult for the guidewire or protection devices alone Therefore, the occlusion of VA origin was initially crossed with a microcatheter (Excelsior SL-10, Stryker Neurovascular, Fremont, CA, USA) and microwire (Asahi Chikai14, Asahi Intecc, Nagoya, Aichi, Japan) (Fig. 1F). Hereafter, the microcatheter was replaced by a balloon catheter (Gateway 2.0 mm diameter and 15 mm length, Stryker Neurovascular), with catheter exchange using a long guidewire (Transcend EX floppy 300 cm length, Stryker Neurovascular). Percutaneous transluminal angioplasty (PTA) was performed followed by stenting with a coronary bare metal stent (Integrity; 3.5 mm diameter and 18 mm length, Medtronic, Minneapolis, MN, USA). Finally, VA origin was successfully recanalized (Fig. 1G). Blood was manually aspirated from the guiding catheter during and after balloon inflation to avoid distal embolism. No distal emboli were detected post-stenting. Next, a microcatheter was navigated intracranially through the stent and fibrinolysis with urokinase (total 24,000 IU) was performed for BA thrombus. Mechanical thrombectomy was not selected because of the inaccessibility. The guiding catheter was not stable in the subclavian artery and it seemed to be difficult to navigate the guiding catheter for thrombectomy through the stent placed at VA origin. Fibrinolysis was moderately effective although BA thrombus still partially remained (Fig. 1H, I). The operation was finished reluctantly because 3 hours had passed after starting intervention and approximately 5 hours after arrival at the hospital.
Postoperative Course
Dual antiplatelet therapy with 100 mg aspirin and 75 mg clopidogrel daily was administered, and anticoagulant therapy with intravenous argatroban was continued for 1 week. The patient's symptoms did not deteriorate after intervention, and all his symptoms were gradually improved postoperatively during the hospitalization. Finally, he left the hospital for rehabilitation 4 weeks later because dysarthria and left hemiparesis still remained. NIHSS at discharge was 5. And modified Rankin Scale score at 3 months was 3.
A follow-up MR image was obtained 1 week later. MR DWI disclosed a high-intensity area around the right SCA territory and the left cerebellar hemisphere mainly fed by the distal part of the left AICA. MR DWI high-intensity area around brain stem was not enlarged postoperatively in comparison with preoperative MR image. MRA demonstrated no re-occlusion of the VA origin and showed clear visualization of the right VA, BA and left SCA despite poor visualization of the distal right SCA (Fig. 1J).
DISCUSSION
Etiology
Atherosclerotic occlusive disease of VA most commonly affects the origin and proximal portion of the VA [1]. Extracranial VA occlusive disease seemed to be mostly made up of benign lesions, the cause of which was attributed to: (1) the capacity to develop collateral reconstitution of the extracranial VA; (2) the usual presence of two viable arteries that join together intracranially, so that if one became compromised, the contralateral artery could compensate adequately; and (3) the slow development of luminal compromise by atherosclerotic plaques, allowing time for collateral development [6].
This article demonstrated a case of stroke due to an acute VA origin occlusion associated with hypoplastic contralateral VA, which led to BA thrombosis, successfully treated by PTA with stenting and intracranial fibrinolysis. As you may know, there were a number of reports about acute occlusion at the cervical portion of the internal carotid artery (ICA) due to atherosclerosis steno-occlusive disease. Cervical ICA occlusion often has concomitant intracranial occlusion [7], which might be brought on by distal migration of a clot from the occlusion site and/or cerebral hypoperfusion due to large vessel occlusion. Acute VA origin occlusion must be closely similar to cervical ICA occlusion. The distal migration of a clot and/or acute hemodynamic insufficiency induced thrombus at BA. In this case, contralateral VA was hypoplastic, consequently, intracranial flow of VA/BA became insufficient, and might have induced the thrombus formation of BA.
Intervention
The current literature has demonstrated the safety and efficacy of PTA with stenting for VA origin stenosis. However, the cases almost all involved the non-acute period [8, 9]. Lin DDM and colleagues reported six cases of acute-subacute posterior circulation strokes due to VA origin occlusion/near occlusion or preocclusive stenosis associated with intracranial thrombosis. In all six cases, PTA with stenting and intracranial thrombolysis was performed as in the present case. Four of six (67%) patients had excellent immediate recovery, whereas two patients expired, one of whom presented with coma at outset [5]. This result indicated that endovascular intervention might be a useful treatment option.
The concerns with the endovascular approach for this setting include two cautions. First, the difficulty in penetrating and navigating the devices across the occlusive site. It carries the risk of iatrogenic dissection or perforation of VA caused by a stray wire-tip. In the present case, a microcatheter and a microguidewire were used to raise the support and tractability for crossing the occlusion site. Second, the risk of distal migration of clots or debris into the intracranial arteries. In the present case, distal embolism did not occur, even though an embolic protection device was not used because of time limitation. However, the previous literature revealed that an embolic protection device might be useful for preventing intracranial embolisms during procedures. Iwata et al. [10] have described the use of flow reversal to prevent distal embolization during the treatment of VA origin chronic occlusion, which was similar to that reported in carotid revascularization procedures.
For the treatment of intracranial lesion, fibrinolysis is convenient regarding the distal accessibility. Mechanical thrombectomy is one of the treatment choices if the access of devices is feasible.
 XML Download
XML Download