

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Congenital diaphragmatic hernia (CDH) occurs at an incidence of 4 per 10,000 live births [1]. Right congenital diaphragmatic hernia (RCDH) occurs less frequently than left congenital diaphragmatic hernia (LCDH), accounting for 10% to 15% of all cases of CDH [2]. The main prognostic factors for CDH are pulmonary hypoplasia and the existence of liver herniation. The current literature on the prognosis of CDH indicate that RCDH is associated with a lower survival rate than LCDH because the vast majority of RCDH cases have liver herniation and, therefore, exhibited more severe pulmonary hypoplasia than LCDH [345]. Herein, we describe a rare case of RCDH that was diagnosed prenatally, in which intrathoracic impaction of the kidney may have protected against further herniation of abdominal contents into the thoracic cavity. To the best of our knowledge, this is the first report of a prenatal diagnosis of RCDH with an intrathoracic kidney alone.
Case report
A 29-year-old multigravida patient who was 32 weeks pregnant was referred to our center because of a fetal ectopic intrathoracic kidney. Her past medical history and family history were unremarkable. She had not taken any medications during her pregnancy. Initial ultrasonography demonstrated a singleton female fetus with appropriate growth for its gestational age, but the right kidney was absent in the ipsilateral renal fossa, whilst the right lower thorax contained a mass with mixed echogenicity, suggesting an ectopic kidney (Fig. 1A).
The left normal kidney and right ectopic one appeared to be of a similar size. Fetal echocardiography showed a mesocardia, a rotation of the fetal heart with the apex of the heart located in the mid-thorax with a structurally normal heart, and no signs of cardiac compression (Fig. 1B). Left lung area to head circumference ratio was 2.54. There were no other abnormalities observed. Follow-up ultrasonography before delivery demonstrated a similar appearance of the intrathoracic kidney without any herniation of the abdominal contents. A female infant was delivered vaginally at 39.0 weeks of gestation with a birth weight of 3,230 g and Apgar scores at 1 and 5 minutes of 6 and 9, respectively.
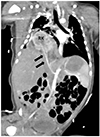
Chest computed tomography at the 2nd day of birth showed a posterolateral herniated right kidney in the neonatal chest with no evidence of herniation of the abdominal viscera. The right renal artery was stretched to feed the intrathoracic kidney (Fig. 2).
At 7 days after birth, repair of the CDH was performed. There was 5 cm defect in the right diaphragm and only the ectopic kidney was herniated through this defect. The ectopic kidney was carefully reduced to the retroperitoneal cavity and the defect was repaired using a commercially available patch. The infant was discharged on day 26 after birth and a postoperative Tc-99m dimercaptosuccinic acid renal scan demonstrated symmetric renal function of 57% (left kidney) and 43% (right kidney). At the 15 month follow-up, the infant was doing well.
Discussion
An intrathoracic kidney is the rarest developmental anomaly among all ectopic kidneys with a prevalence of less than 0.01% [6]. Most patients are diagnosed incidentally, even in adults, because this disorder is asymptomatic. A prenatal diagnosis of ectopic intrathoracic kidney combined with CDH has only rarely been reported, with just five described cases to date [7891011]. We here present the first case of a prenatally diagnosed intrathoracic kidney that prevented herniation of other abdominal contents, including the liver, in a fetus with RCDH. An underlying CDH should always be suspected in cases of intrathoracic kidney, as this condition may manifest later, either prenatally or postnatally [8].
The prognosis of prenatally diagnosed intrathoracic kidney combined with CDH remains unclear because of the small number of cases. Postnatal outcomes were encouraging in all five previously reported cases, as well as in our current case. Intrathoracic kidneys usually function normally and no surgical treatment is required without an associated anomaly. One of the important causes for a favorable outcome would be a protective effect of the intrathoracic ectopic kidney. Herniation of fewer abdominal contents into the thoracic cavity as a consequence of impaction of a kidney, which would act as an anatomical barrier, might allow for better development of both lungs throughout the pregnancy.
The prenatal diagnosis of RCDH remains much more difficult than that of LCDH [1]. The ultrasonographic findings of LCDH are intrathoracic cystic lesions with a mediastinal shift to the right side and the absence of a fluid-filled stomach in the normal position. By contrast, the liver is commonly herniated into the thoracic cavity in RCDH and by analogy in ultrasonographic echogenicity between the liver and lung, it would be difficult to diagnose RCDH prenatally. The diagnostic clues of RCDH include portal blood flow, ascites, or positioning of the gallbladder in the thoracic cavity [412]. As in our present case, an intrathoracic kidney could be also a diagnostic clue for the diagnosis of RCDH [10]. The ultrasonographic finding was the absence of a kidney in the renal fossa with a mixed echogenic mass in the ipsilateral thoracic cavity, resulting in a mediastinal shift. Color Doppler could demonstrate an abnormal course of the renal artery entering the fetal thorax to feed the intrathoracic mass [10]. In our present case, an upwardly stretched renal artery observed by postnatal computed tomography helped to diagnose intrathoracic kidney associated with RCDH.
The clinical outcomes for fetuses with CDH may be improved by fetal endoscopic tracheal occlusion (FETO) with balloon [13]. FETO might improve lung development as a result of the expansion of the fetal lungs by collecting pulmonary secretions and stretching the tissue. However, even in a comparison of outcomes following FETO versus expectant management, no significant difference in the survival of RCDH cases was detected, although this might be be a consequence of the small number of cases [2].
We propose several explanations for why the outcome of RCDH appears to be poorer than that of LCDH with a similar prenatal lung volume. First, herniation of liver, which is almost always present, is perceived as an indicator of a poor prognosis, although the significance of this finding has only been shown for LCDH [2]. Second, the right lung normally accounts for 57% of the total functional lung volume, so any developmental abnormality of the right lung may have a bigger clinical impact [2]. Third, the size of defect necessary to permit herniation of the liver on the right side is likely to be substantially larger than that of a LCDH. This could explain the higher rate of patch repair for RCDH [1], as was observed in our case.
Several studies have described poorer postnatal outcomes in RCDH compared with LCDH [235], whereas others have found no difference between them [1415]. We suggest two reasons for the difficulties in evaluating the prognosis of RCDH. First, this condition is rare. Compared with LCDH, the current literature on prognostic factors and outcomes associated with RCDH contain inconclusive data because of the rarity of this condition. Second, herniation of the liver can be involved. Liver herniation and the lung-to-head ratio have been recognized as prognostic factors in all cases of CDH. Although significance has only been shown for LCDH, herniation of the liver may indicate a larger defect and therefore a poorer outcome [2]. As most fetuses with RCDH have herniation of the liver, this finding could not be a significant prenatal prognostic factor in RCDH. Similarly, the utility of lung-to-head ratio measurements for predicting survival in RCDH is controversial [4]. Hence, another prenatal prediction model that can differentiate RCDH from LCDH may be needed.
In conclusion, cases of intrathoracic ectopic kidney with RCDH are extremely rare, but this condition could represent a protective barrier that can prevent herniation of abdominal viscera including liver and parents should be counseled about the good prognosis even in RCDH.

 XML Download
XML Download