

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
During the process of long bone measurement, locating the precise anatomic plane to perform ultrasound biometry and reducing inter- and intra-operator measurement error are critical for diagnosis. With respect to fetal ultrasound, the biometry of the fetal femur is technically simple due to the one-dimensional nature of the measurement. However, unlike the proximal extremities, the long bones of the distal areas can be difficult to measure. For example, in the distal upper and lower limbs, radius and ulna, and tibia and fibula, the paired bones are located too close together for proper differentiation. Other exacerbating factors, including constant fetal movements, the consequent variation in fetal position, degree of the expectant mother's obesity, quantity of the amniotic fluid, and location of the placenta further aggravate the difficulty in making proper measurements.
In conventional two-dimensional (2D) ultrasound, the sonographer must manipulate the transducer accordingly to locate an appropriate plane for fitting measurements. The 2D-ultrasound is also burdensome as sonographers must meet with patients directly to conduct a lengthy examination. Furthermore, the accuracy of diagnosis and construction of images mainly depend on the degree of the sonographer's experience and expertise. However, the newer three-dimensional (3D) ultrasound scans volume data in a short period of time and reconstruct a 3D image, which can be cut into multiple sections for further manipulation to obtain precise plane much like the saved images of computed tomography or magnetic resonance imaging. 3D-ultrasound is also particularly useful in that the saved images allow diagnostic deliberation by the sonographer even after the examination ends and the patient is unavailable for further testing. Recently published studies have verified the utility of 3D-ultrasound in various diagnostic areas, including fetal biometry, skeletal dysplasia, facial anomaly, and fetal echocardiography [12345]. However, 3D-ultrasound also requires the manipulation of 3D volume data to reconstruct the images, which requires time and effort. Furthermore, such manipulation efforts also depend on the expertise and experience of the sonographer.
To compensate for these weaknesses, long bone automated detection system, five-dimensional 5D Long Bone (5D LB) was made available to streamline the process of reconstructing the lower limb long bone images and performing fetal biometry. The present study compared the biometric data of conventional 2D-ultrasound, manually manipulated 3D volume data, and 5D LB-treated 3D volume data to determine the feasibility of 5D LB functions in light of other available methods.
Materials and methods
1. Study population
This study was performed with 39 pregnant women with singleton pregnancies at 26+0 to 32+0 weeks of gestation who visited the Department of Obstetrics at the Yonsei University Health System between November 2011 and August 2012. Subjects with fetal abnormality was suspected on ultrasound examination, those who had a medicosurgical disease, or multiple pregnancies were excluded from the study. This study was approved by the institutional review board and informed consent was obtained from all the participants.
2. Lower limb long bone length measurement
One experienced operator (operator 1, a maternal-fetal medicine clinical instructor) and one inexperienced operator (operator 2, two gynecology residents) participated in the ultrasound examination. Every 2D and 3D ultrasound examination was performed twice, once by the inexperienced operator and again by the experienced operator. Each ultrasound scanned the proximal (femur) and distal (tibia and fibula) areas of the long bones of the right lower limb. For the measurement, the Accuvix V20 Prestige (Medison Co., Seoul, Korea) was used. For 2D-ultrasound measurements, a 2-6 MHz transabdominal ultrasound transducer was used and 3D volume data were acquired using a 4-8 MHz volume transducer.
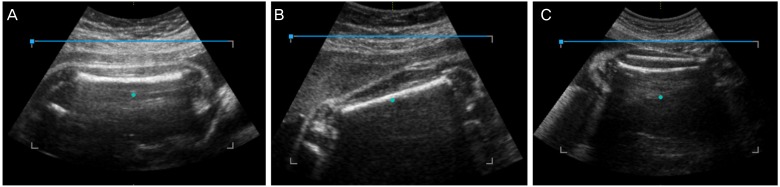
For 2D-ultrasound measurement, the transducer was aligned to the long axis of the diaphysis, and the image was captured and used to measure the length. To obtain 3D volume data, the entire bone length of the femur was identified on the screen, as in the 2D-ultrasound measurement, and the long axis of the femur was placed in the direction of the x-axis in the image in which the ultrasound beam was perpendicular to the bone. The femur was included in the volume box such that the bone length occupied about 80% of the entire image, and the volume data were captured using 3D scanning (Fig. 1A). These data were designated the longitudinal-90 (long-90) set. Then, the femur was rotated clockwise or counterclockwise by 45 degrees on the screen, and the volume data were again captured using 3D scanning (Fig. 1B). These data were designated the longitudinal-45 (long-45) set. The distal lower extremity bones, i.e., the right tibia and fibula, were measured similarly: the entire bone length was identified on the screen, the long axis of the bones was placed in the direction of the x-axis in the image, as was femur long-90 and the volume data were captured using 3D scanning (Fig. 1C).
The 3D-ultrasonograph long bone length was measured offline by a maternal-fetal medicine specialist (JYK) who had not participated in the ultrasonograph measurements. The acquired volume data were reconstructed in a multiplanar mode to adjust the x, y, and z-axes of each plane. Then, an appropriate plane was located for the long bone length measurements of the right lower limb.
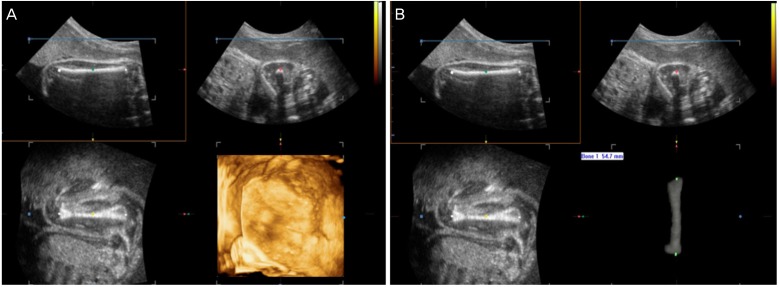
Subsequently, the long bone length was measured using the 5D LB with the following procedures. The volume data used in the manual 3D-ultrasound measurement were displayed in an offline multiplanar mode, and the 5D LB set key was pressed on the system, wherein the system automatically analyzed the 3D volume data, reconstructed the 3D image of the long bones, and displayed the measured lengths of the long bones on the screen (Fig. 2).
3. Statistical analysis
Statistical analysis was performed using the PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA) and MedCalc ver. 12.7 (MedCalc Software, Ostend, Belgium). The Kolmogorov-Smirnov test was used to test the normal distribution of the measurement data. The paired t-test was performed to analyze intra- and inter-observer variability. Agreement was analyzed by using Bland-Altman plot, Passing-Bablok regression and calculating the interclass correlation coefficient (ICC). P-value of <0.05 was considered statistically significant.
Results
To measure the length of the fetal femur, tibia, and fibula using different methods, two operators performed 2D- and 3D-ultrasound examinations with a total of 39 subjects two times each. Of the 624 total 5D LB measurements, the overall success rate was 86.2% (538/624); the overall failure rate, 8.3% (52/624); and the overall error rate, 5.4% (34/624). For the femur, the success rate of long-90 measurement was 91.0% (142/156) and that of long-45 measurement was 96.1% (150/156). As such, the long-45 success rate was slightly higher than that of the long-90. The success rate was lower for the measurements of the tibia (80.7%, 126/156) and fibula (76.9%, 120/156), in which the length of both bones was measured simultaneously, than for the measurements of the femur (Table 1).
To examine the variation in the long bone length measurements depending on the volume scanning angles in the 3D-ultrasound, the variability and agreement were analyzed between the femur long-90 and femur long-45 measurements obtained by manual 3D-ultrasound and 5D LB. As shown in Table 2, neither 3D-ultrasound nor 5D LB exhibited a significant difference in measurement values between the different scanning angles. In fact, the scanning angles exhibited an ICC >0.9, showing a high level of agreement. Consequently, long-90 data were used in all subsequent analyses.
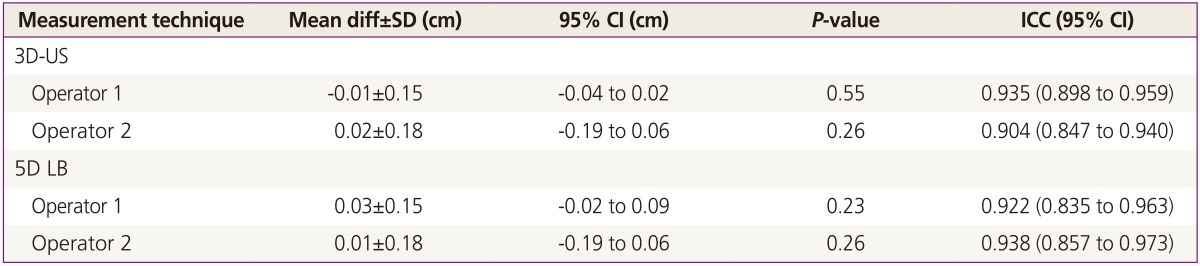
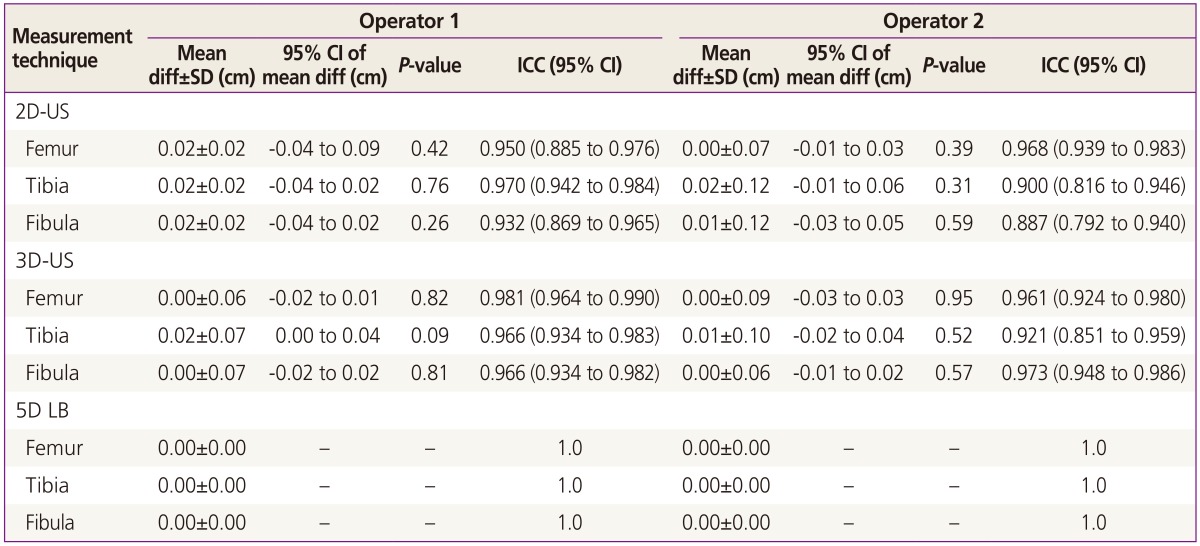
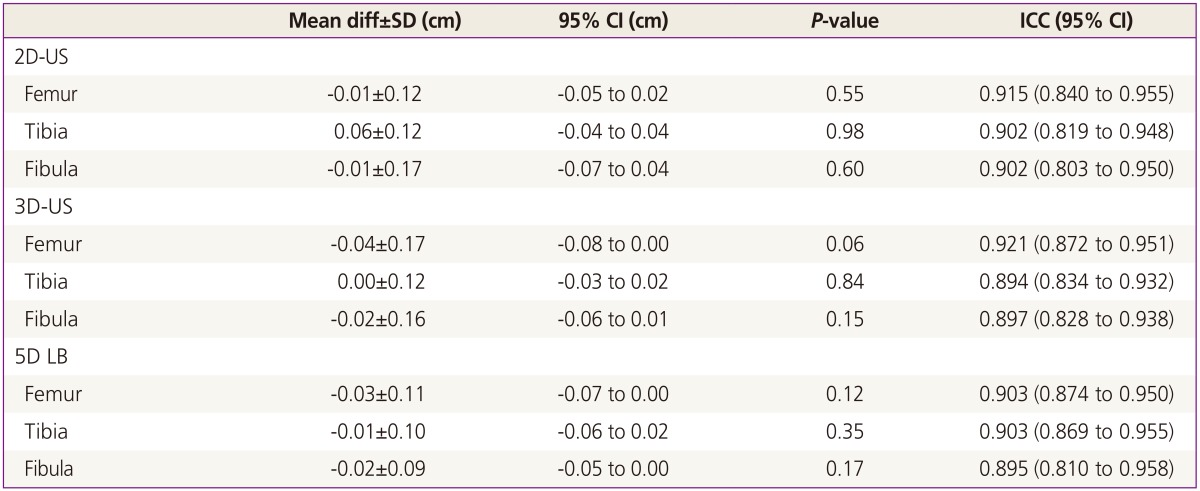
The intra- and inter-observer variability and reproducibility were analyzed with respect to the three measurement methods, and the results showed no significant differences among the methods; in fact, a rather high degree of agreement was noted (Tables 3, 4).
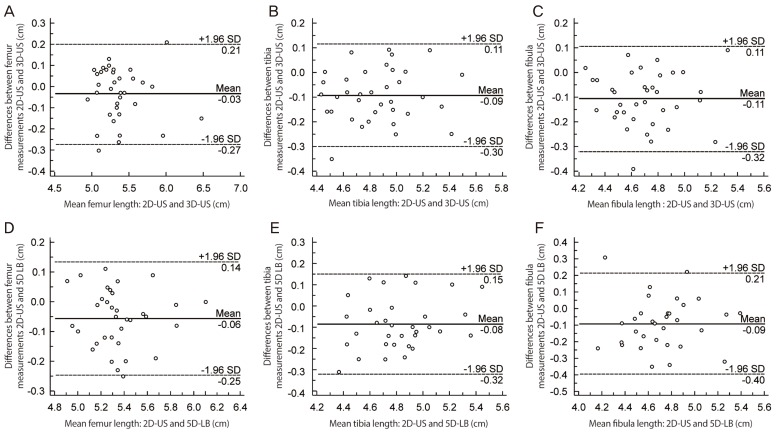
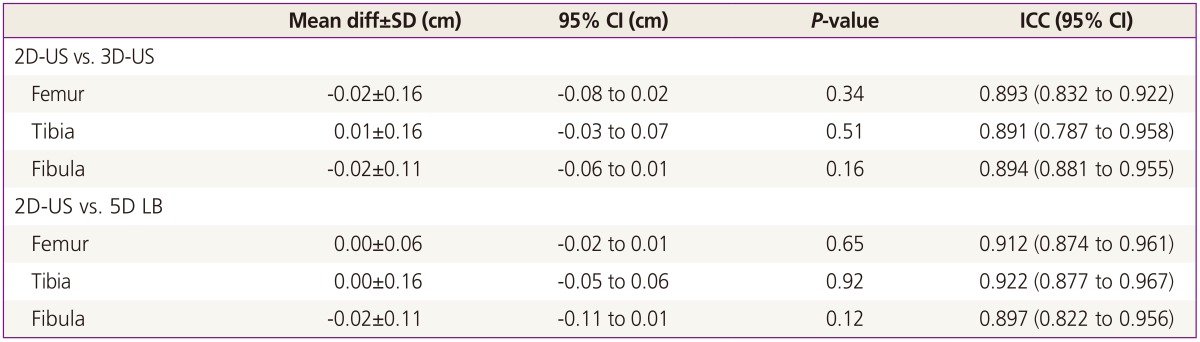
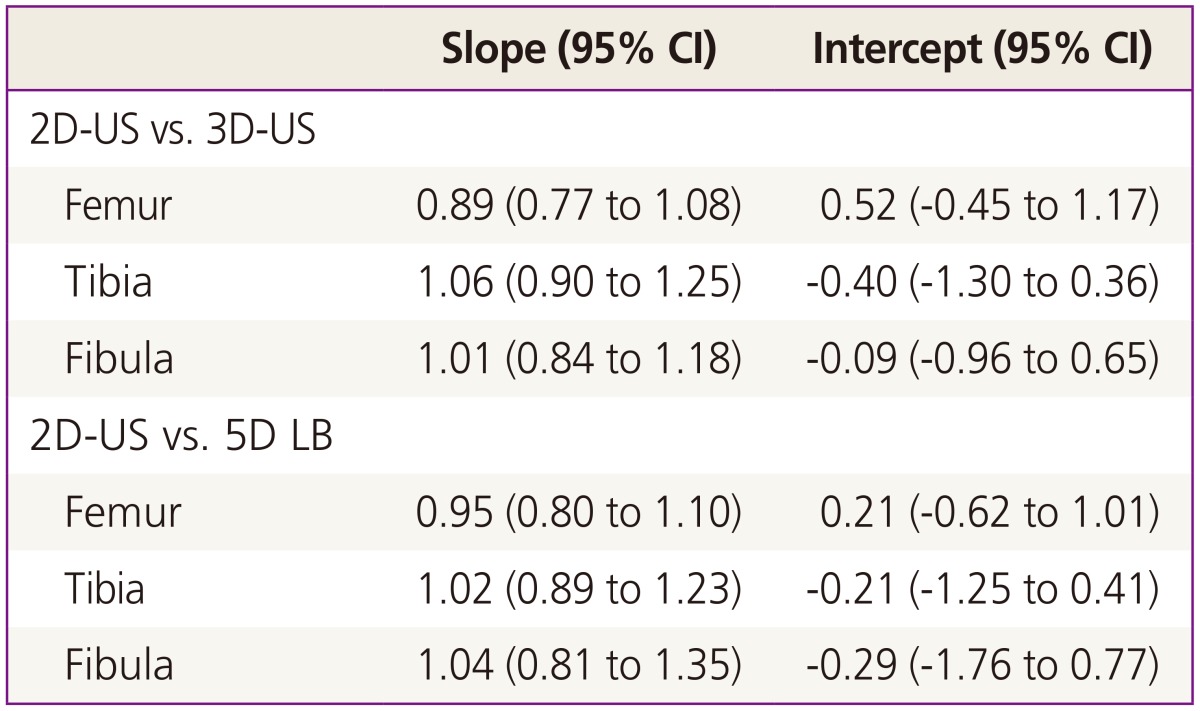
Then, the measurement values of 3D-ultrasound and 5D LB were compared with the standard 2D-ultrasound measurement values to verify the reproducibility of the two former methods. When the 3D-ultrasound and 5D LB methods were compared with the 2D-ultrasound, the measurement values did not exhibit a significant difference. The ICC was >0.89 and the Bland-Altman plot showed an even distribution near zero (Table 5, Fig. 3). Passing-Bablok regression showed no significant systemic or proportional differences (Table 6).
Discussion
Ultrasound examination can be safely applied to women of childbearing age or pregnant women because it does not use ionizing radiation and is able to obtain real-time tomograms of any region depending on the position at which the sonographer places the probe. In addition, the newer 3D-ultrasonograph method can reconstruct the images from saved volume data to enable the sonographer to analyze the images in various sections even after the patient leaves the examination room. In other words, only a single scan is required to provide sufficient data for in-depth analysis. Even better, the recent development of an automated 3D-ultrasound further reduces the time and effort required to manually manipulate the volume data by automatically reconstructing images from the scanned volume data through a preloaded program on the apparatus.
Volume imaging through 3D-ultrasound is useful since the desired image may be reconstructed by manipulating volume data acquired by volume sweeping even if the correct plane is not found at the time of examination. Benacerraf et al. [5] reported that volume data were acquired within 2 minutes and interpreted in 6 to 7 minutes using 3D-ultrasound in the standard fetal anatomic survey, indicating that the temporal efficiency of the 3D-ultrasound was greater than that of 2D-ultrasound, which took 19.6 minutes. They also reported that 3D-ultrasound may be useful in fetal anatomic surveillance because it allows for tomographic imaging study, like computed tomography or magnetic resonance imaging.
Acquired 3D volume data can be displayed in three orthogonal planes and provide all the 2D planes for a complete anatomical evaluation of the particular organ. Therefore, 3D-ultrasound with multiplanar reconstruction or surface rendering has advantages in the evaluation of complex anatomy, such as fetal heart, central nervous system and face [678910]. For example, a single volume sweep provides reconstruction of a midsagittal plane for evaluation of nuchal translucency and nasal bone [1112]. From 3D fetal echocardiography, standardized planes and intracardiac structures of the fetal heart can be reconstructed from volume data in real time. Spatiotemporal image correlation enables an automated volume acquisition of the fetal heart by using a mechanical volume transducer and software. Real-time three-dimensional echocardiography is another kind of technology using a matrix array transducer which can display the fetal heart in real time. Furthermore, 3D-ultrasound provides the ability to store volume data that can be manipulated after the patient has left the examination room and also be transmitted electronically to evaluate elsewhere.
Despite these advances of 3D-ultrasound, the manipulation of volume data requires a learning curve and is also operator dependent. Automated 3D imaging will allow an operator independent and standardized approach to evaluate complex anatomical evaluation and improve the efficiency by reducing the time to complete the ultrasound examination.
Buoyed by the recent advancements in ultrasound technology, numerous studies have been conducted to develop a more efficient and precise automated ultrasound system for biometry. Zador et al. [13] performed automated measurements of the biparietal diameter, occipitofrontal diameter, and head circumference using a personal computer-based system. The results showed that the automated measurements not only were highly correlated with the measurements taken by an experienced sonographer using conventional methods but also decreased the amount of time needed to make the measurements available for analysis. Thomas et al. [14] conducted computerized measurements of the femur and humerus. Other studies have verified the feasibility of computerized automated fetal biometry measurement and its good intra-interobserver variability [1516].
Ultrasound diagnosis based on automated computerized systems can be considered semi-automatic, since the operator searches for the correct plane and the computer performs the automated caliper placement through image subtraction. Thus, the ultimate goal is to create a fully automated system, in which the correct plane is also determined by the instrument.
The present study is significant in that it verified the feasibility of automated long bone length measurements through 5D LB system. Our study focused on gestational ages of 26 to 32 weeks to assist less experienced operator in avoiding falsely including the triangular spur artifacts and the distal femoral epiphysis in the late trimester; 20 weeks long bone measurement is quite straight forward as only the diaphysis is seen and to facilitate multiple long bone measurements. In a fetus with suspected skeletal dysplasia, measuring all of the long bones may be cumbersome and skeletal dysplasia (or long bone shortening) usually manifests in the late 2nd to 3rd trimester.
The volume sweep initiated by the automated long bone detection system only takes a few seconds to perform and the acquired volume data are available for offline manipulation. Such processes decrease the duration of the examination period, reduce the incidence of musculoskeletal stress-induced injuries common among sonographers [1718], and construct a more precise image plane by being less affected by the movement or position of the fetus. In addition, the manual volume data manipulation required by 3D-ultrasound was replaced by an automated system that enables the manipulation to be completed in just a few seconds. In our study, volume sweep takes 2 seconds with sweep angle of 30 degrees and software execution to measurement output takes 4 seconds.
Nonetheless, biometric measurement using 5D LB still requires improvement. In this study, the overall success rate of 5D LB measurements was 86.2% (538/624), the overall failure rate was 8.3% (52/624), and the overall error rate was 5.4% (34/624). Among the above measurements, the femur long-90 and femur long-45 exhibited a relatively high success rate of 91.0% (142/156) and 96.1% (150/156), respectively. However, the tibia and fibula length measurement exhibited lower success rates at 80.7% (126/156) and 76.9% (120/156), respectively. Although it is estimated that the femur long-90 has highest success rate theoretically, the femur long-45 has slightly higher than long-90. Based on 4 cases that had failed, the thigh was abutting uterine wall without space filled with amniotic fluid between the wall and the thigh, thus the software was unable to differentiate bright bone outline and high echogenic skin line. However, when the femur was at 45 degrees-angle of inclination, there was amniotic fluid pocket thus less error for the software in selecting out bone outline.
Some of the reasons for 5D LB measurement failures include failure to locate the appropriate sagittal plane to construct an image of the long bone, misplacement of the caliper due to the unusually high soft tissue echo near the target long bone, unclear differentiation between the bone and soft tissue due to the low bone echo, image blurring due to fetal movements or maternal obesity, and acoustic shadowing due to the obstruction of nearby organs or the position of the two long bones. Such measurement errors have been reported since conventional 2D-ultrasound was first used. While volume data manipulation has made strides in rectifying some of the measurement errors, such measurement errors still occur in 3D-ultrasound examination [19]. These errors need to be eliminated, perhaps by compensation using the 5D LB system algorithm.
Ultrasound is highly operator dependent thus the quality of ultrasound examination can vary accordingly. In hope to aid in standardization and reduce operator dependency, software that semi-automatically or automatically reproduce 2D image plane or measurement using 3D volume data was developed and has been promising [679101112]. But limitation lies in that with current ultrasound machine that enables us to perform 2D- and 3D-ultrasound using two separate transducers, adding 3D software may not be practical but rather cumbersome and time-consuming since we need to switch back and forth between functions to apply the 3D software. Thus, automated femur measurement software by itself may not be attractive at present setting, however, ultrasound technology is innovating towards combining 2D and 3D transducer functions [202122] which will allow integration of multiple 3D software with realtime scanning in a most practical way. In such future perspective on where ultrasound technology is heading, 5D LB function should serve as one of gateway to automated biometry software.
The present study performed a comparative analysis of the feasibility of the 5D LB program with respect to its fetal long bone length measurement capacity. The capacity of the 5D LB program was compared with that of the conventional 2D- and 3D-ultrasound. Fetal lower limb long bone measurement using 5D LB demonstrated low intra and -inter-observer variability and a high level of agreement compared with data acquired using the conventional imaging techniques. As such, the 5D LB program exhibited high feasibility with respect to its capacity to perform fetal biometry. However, further improvements on the measurement failures and errors must be made for 5D LB to replace conventional 2D-ultrasound fetal biometry. Through this process, more efficient and precise ultrasound diagnosis will be possible.

 XML Download
XML Download