

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sertoli-Leydig cell tumors (SLCT) belong to the group of sex cord-stromal tumors of the ovary and account for approximately 7% of all ovarian malignancies [1]. Surgery remains the cornerston of initial treatment for SLCTs, and since the 1980s, platinum-based chemotherapy has been the most widely used postoperative treatment [2]. Recurrence and metastases beyond the ovary or into the upper abdomen is rare and malignant SLCT tend to relapse early within 2 to 3 years [2]. Due to their rarity, limited data are available regarding a role of chemotherapy in the management of SLCTs.
We describe a case of recurrent ovarian SLCT whose salvage treatment was successful with paclitaxel and carboplatin chemotherapy.
Case Report
A 57-year-old multiparous woman presented with abdominal distension for one year. Her menopause was at 50 years of age. On physical examination, the abdomen was distended with a large pelvic mass. A computed tomography (CT) scan of the abdomen and pelvis revealed a 16.0×11.5 cm complex cystic and solid pelvis. Laboratory tests revealed an elevated serum CA-125 (113.5 U/mL). Other tumor markers including α-fetoprotein, lactate dehydrogenase, carcinoembryonic antigen and CA-19-9 were within the normal range.
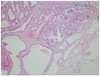
An exploratory laparotomy was performed with findings of a mobile complex left ovarian mass, and no evidence of disease spread. Frozen biopsy revealed sex-cord stromal tumor. A total abdominal hysterectomy with bilateral salpingo-oophorectomy, peritoneal cytology, total omentectomy, incidental appendectomy, peritoneal biopsy, and pelvic and para-aortic lymph node dissection was performed. The permanent histopathologic exam confirmed a Sertoli-Leydig cell tumor of the left ovary, with intermediate differentiation and retiform elements (Fig. 1). The right salpinx was involved by the tumor cells and the peritoneal cytology was positive for tumor cells. Preoperative and postoperative hormone studies were within the normal range. The patient received three cycles of chemotherapy with bleomycin, VP16, and cisplatin. After eight months, a follow-up CT showed a newly developed irregularly-shaped mass around the hepatic flexure. The serum CA-125 level was 42.32 U/mL. She received twelve cycles of chemotherapy with paclitaxel and carboplatin. A CT scan after completion of the second-line chemotherapy showed complete remission of the recurrent lesion and the serum CA-125 level returned to the normal range. The patient was started on follow-up visits, and the patient was disease-free 51 months after completion of salvage treatment.
Discussion
The malignant potential of SLCTs is nearly absent in well differentiated tumors, approximately 11% in the intermediate type, 59% in poorly differentiated tumors, and approximately 19% in tumors with heterologous elements [2]. Survival is favorable in better differentiated tumors. Most of the tumors were stage I at the time of presentation, even if of the poorly differentiated type [2]. Recurrence and metastasis occurs in 12% to 22% of cases. The mortality rates vary from 12% to 34% [3]. Our case was initially stage IIIA and showed relapse eight months after primary treatment. These tumors are more often encountered in young women before 40 years of age [1] and often manifest endocrine symptoms or sign such as defeminization, followed by masculinization [3]. However, our case was postmenopausal woman and had no endocrine manifestation.
Surgery is standard treatment of SLCTs. In patient with stage IA disease, unilateral salpingo-oophorectomy is the treatment of choice. In older women or patients with advanced stage, removal of the uterus, ovaries, omentum and the metastatic tumors are considered to be standard procedures [4]. The value of postoperative adjuvant therapy has not been proven [5]. According to the current literature, three or four cycles of adjuvant chemotherapy with bleomycin, etoposide, and cisplatin or cisplatin, dactinomycin and cyclophosphamide are recommended in intermediate or poorly differentiated tumors, or in patients with advanced disease [6].
Management of recurrent SLCTs usually poses a therapeutic challenge because of the lack of experience in managing patients due to the rarity of the disease. In cases with evidence of local recurrence, further surgery should be considered which, in cases with metastasis, should be followed by chemotherapy or irradiation. A combination of vincristine, actinomycin D, and cyclophosphamide has been tried and second-line chemotherapy drugs are bleomycin, and cisplatin [7,8]. Some investigator has been reported the effect of taxane and platinum combination chemotherapy in patients with SLCTs [9]. Our case completely responded to 2nd-line chemotherapy with paclitaxel and carboplatin after recurrence. However, most peer-reviewed reports of the use of chemotherapy are of single patient experience, or small series. There are no randomized trials in the medical literature involving the administration of chemotherapy for ovarian stromal tumors.
In conclusion, in case with advanced stage or metastatic SLCTs, cytoreductive surgery and postoperative chemotherapy should be performed and chemotherapy should be considered on recurrence. Our case showed successful response by salvage chemotherapy with paclitaxel and carboplatin on recurrent SLCT.
 XML Download
XML Download