

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
To compare the outcomes of single port access (SPA) laparoscopic hysterectomy and conventional laparoscopic hysterectomy for the large uterus of more than 500 g.
Methods
Twenty-seven cases of SPA laparoscopic hysterectomy and 32 cases of conventional laparoscopic hysterectomy were retrospectively analysed. The surgery had performed by single surgeon from January 2010 to July 2011 in Chungnam National University Hospital. We compared demographic characteristics and surgical outcomes.
Results
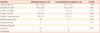
There were no significant difference in patients' age, body mass index, past surgical history, postoperative additional pain control and duration of hospital stay between the two groups. Uterine weight was 706.5±363.2 g (range, 500-2,415 g) for SPA laparoscopic hysterectomy and 634.0±153.3 g (range, 500-1,130 g) for conventional laparoscopic hysterectomy and significantly not different between the two groups. Operation time was significantly longer in SPA laparoscopic hysterectomy than conventional laparoscopic hysterectomy (81.1±18.1 minutes vs. 67.2±16.8 minutes). Postoperative change in hemoglobin and hematocrit was statistically higher in SPA laparoscopic hysterectomy than conventional laparoscopic hysterectomy (1.9±0.9 g/dL, 2.9±4.2% vs. 1.0±1.3 g/dL, 6.2±2.9%, respectively).
Conclusion
Operation time was longer and postoperative change in hemoglobin and hematocrit was significantly higher in SPA laparoscopic hysterectomy than conventional laparoscopic hysterectomy. However, SPA laparoscopic hysterectomy will replace conventional laparoscopic hysterectomy in a future with improving surgical technique.
Figures and Tables

References
1. Reich H, DiCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989. 5:213–216.
2. Quiñones GR, Alvarado DA, Ley Ch E. Tubal ligation using Yoon's ring. Ginecol Obstet Mex. 1976. 40:127–136.
3. Pelosi MA, Pelosi MA 3rd. Laparoscopic hysterectomy with bilateral salpingo-oophorectomy using a single umbilical puncture. N J Med. 1991. 88:721–726.
4. Podolsky ER, Rottman SJ, Poblete H, King SA, Curcillo PG. Single port access (SPA) cholecystectomy: a completely transumbilical approach. J Laparoendosc Adv Surg Tech A. 2009. 19:219–222.
5. Canes D, Desai MM, Aron M, Haber GP, Goel RK, Stein RJ, et al. Transumbilical single-port surgery: evolution and current status. Eur Urol. 2008. 54:1020–1029.
6. Kommu SS, Kaouk JH, Rané A. Laparo-endoscopic single-site surgery: preliminary advances in renal surgery. BJU Int. 2009. 103:1034–1037.
7. Romanelli JR, Roshek TB 3rd, Lynn DC, Earle DB. Single-port laparoscopic cholecystectomy: initial experience. Surg Endosc. 2010. 24:1374–1379.
8. Canes D, Berger A, Aron M, Brandina R, Goldfarb DA, Shoskes D, et al. Laparo-endoscopic single site (LESS) versus standard laparoscopic left donor nephrectomy: matched-pair comparison. Eur Urol. 2010. 57:95–101.
9. Teixeira J, McGill K, Binenbaum S, Forrester G. Laparoscopic single-site surgery for placement of an adjustable gastric band: initial experience. Surg Endosc. 2009. 23:1409–1414.
10. Moris DN, Bramis KJ, Mantonakis EI, Papalampros EL, Petrou AS, Papalampros AE. Surgery via natural orifices in human beings: yesterday, today, tomorrow. Am J Surg. 2011. 12. 27. [Epub]. DOI: http://dx.doi.org/10.1016/j.amjsurg.2011.05.019.
11. Paek J, Nam EJ, Kim YT, Kim SW. Overcoming technical difficulties with single-port access laparoscopic surgery in gynecology: using conventional laparoscopic instruments. J Laparoendosc Adv Surg Tech A. 2011. 21:137–141.
12. Paek J, Kim SW, Lee SH, Lee M, Yim GW, Nam EJ, et al. Learning curve and surgical outcome for single-port access total laparoscopic hysterectomy in 100 consecutive cases. Gynecol Obstet Invest. 2011. 72:227–233.
13. Lee M, Kim SW, Nam EJ, Yim GW, Kim S, Kim YT. Single-port laparoscopic surgery is applicable to most gynecologic surgery: a single surgeon's experience. Surg Endosc. 2012. 26:1318–1324.
14. Song T, Kim TJ, Kim MK, Park H, Kim JS, Lee YY, et al. Single port access laparoscopic-assisted vaginal hysterectomy for large uterus weighing exceeding 500 grams: technique and initial report. J Minim Invasive Gynecol. 2010. 17:456–460.
15. Ichikawa M, Akira S, Mine K, Ohuchi N, Iwasaki N, Kurose K, et al. Evaluation of laparoendoscopic single-site gynecologic surgery with a multitrocar access system. J Nihon Med Sch. 2011. 78:235–240.
16. Yim GW, Jung YW, Paek J, Lee SH, Kwon HY, Nam EJ, et al. Transumbilical single-port access versus conventional total laparoscopic hysterectomy: surgical outcomes. Am J Obstet Gynecol. 2010. 203:26.e1–26.e6.
17. Jung YW, Lee M, Yim GW, Lee SH, Paek JH, Kwon HY, et al. A randomized prospective study of single-port and four-port approaches for hysterectomy in terms of postoperative pain. Surg Endosc. 2011. 25:2462–2469.
 XML Download
XML Download