

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis is a common health problem caused by an immune-mediated inflammatory reaction after allergen exposure. It is not a life-threatening condition but in most cases it interferes with the patient's personal life and imposes a substantial burden on public health in economic terms. In the United States, 17-25% of the population, approximately 39 million, is estimated to have allergic rhinitis [1]. The prevalence varies among countries, probably because of geographic and aeroallergen differences [2-5]. For example, one sixth of Canadians suffer from this disorder [6].
In recent years, the worldwide increase in allergic diseases has been associated with low vitamin D. Schauber et al. [7] stated that the association between low serum vitamin D levels and an increase in immune disorders is not coincidental. Growth in populations has resulted in people spending more times indoors, leading to less sun exposure and less cutaneous vitamin D production [8].
Several studies have been designed to investigate the value of vitamin D in the treatment of allergic diseases and asthma, but still the results are controversial [7, 9, 10].
The significant impairment of quality of life and morbidity caused by allergic rhinitis, and the easily-treated vitamin D deficiency with which it may be associated, motivated the design of this study. Herein, the vitamin D status of the study patients with allergic rhinitis was compared to vitamin D levels from the normal population.
MATERIALS AND METHODS
Study design and population
The study included patients with allergic rhinitis, who were referred to the Asthma, Allergy and Clinical Immunology Clinic of the Rasoul Akram Hospital (for routine visits) during a one year period between September 2008 and September 2009. Allergic rhinitis patients were diagnosed clinically using Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 criteria [11] during a medical visit. Expert allergists carried out skin prick test to determine specific IgE sensitivity to common aeroallergens in Iran (outdoor and indoor). The study results of vitamin D serum levels in allergic rhinitis were compared with the results from another study carried out on the normal population to evaluate their vitamin D status [12].
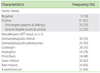
Sixty-nine patients were enrolled to complete a questionnaire that was designed by comparing 15 standard allergy questionnaires and modified to reflect regional characteristics. The questionnaire concerned demographic data, probable risk factors associated with allergic rhinitis, co-morbid diseases, multiple signs and symptoms of disease and the history of patient's medications. Fifty of the original 69 patients were selected for participation in this study.
Exclusion criteria concerned patients who had co-morbid disease in addition to allergic rhinitis that could affect vitamin D serum levels. Such diseases included rheumatoid arthritis, cystic fibrosis, multiple sclerosis, ulcerative colitis, crohn's disease, celiac disease, rickets, osteomalacia, sarcoidosis and thyroid dysfunctions, and individuals who had received medications including corticosteroids, barbiturates, bisphosphonates, sulfasalazine, omega3 and vitamin D components such as calcium-D were excluded.
According to the severity of the allergic rhinitis, patients were classified into mild, moderate and severe groups. Classification was based on the duration of symptoms, interference with daily activities and sleep disturbance; using ARIA 2008 criteria, interpolated in the questionnaires.
Measurements
A two ml blood sample was obtained from the patients to check the vitamin D level. Blood samples were centrifuged and the samples were stored at -70℃ until required. A standard CPBA kit (DRG Instruments GmbH, Germany) was used to measure the 25 (OH) D level. Levels equal to or greater than 37 nmol/L were considered normal. Levels less than or equal to 12.5 nmol/L, levels between 12.5 and 25 nmol/L and levels between 25 and 37 nmol/L were considered to reflect severe, moderate and mild deficiency, respectively [13].
RESULTS
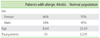
Of the 50 patients enrolled in the study, 17 (34%) were men and 33 (66%) were women. The mean age of the patients was 26.2 ± 1.1 years (range from 8 to 64 years) (Table 1).
A vitamin D level of more than 37 nmol/L was considered normal and lower levels were considered to reflect deficiency. The mean vitamin D level was 31.5 ± 2.5 nmol/L in patients with allergic rhinitis.
The vitamin D level was significantly higher in men than women (46.8 ± 1.2 vs. 26.7 ± 1.9; p = 0.00).
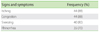
Of the 50 patients evaluated, 17 (34%) were experiencing severe signs and symptoms of the allergic rhinitis, 18 (36%) were considered to be moderate and 15 (30%) were classified as mild. The mean vitamin D level was 29.4 ± 4.7 nmol/L in patients with severe symptoms, and 34.5 ± 4.5 and 30.9 ± 5.9 nmol/L in the moderate and mild groups, respectively. The mean vitamin D level was not significantly different among the three groups (p = 0.7).
There was no significant relationship between vitamin D status, duration and symptoms of allergic rhinitis or the contact time with allergens. (p > 0.05).However, the one sample t-test, showed the prevalence of severe vitamin D deficiency to be significantly greater in patients with allergic rhinitis than in the normal population utilized in the study of Moradzadeh et al. [12] (p = 0.03) (Table 4).
DISCUSSION
Our study identified a few important findings in the growing area of allergy and vitamin D levels. This study demonstrated a significant vitamin D deficiency among females, which could reflect lower sun exposure due to the lifestyle and the type of clothing worn by Iranian women. Severe cases of allergic rhinitis were accompanied by more prominent deficiency in vitamin D, although this was not significantly different from the other two groups. The results demonstrate the importance of assessing vitamin D levels in patients with allergic rhinitis. Few studies have addressed this issue; but an experimental investigation by Pichler et al. [14] reported the immunoregulatory action of vitamin D in the development of Ig-E mediated allergy.
In a study performed by Moradzadeh et al. [12] the mean vitamin D level was measured in 5,329 normal Iranian individuals. The results demonstrated that 27.2% had mild vitamin D deficiency, 42.8% moderate and 5.1% had a severe deficiency. In comparison with the results presented herein, the prevalence of severe vitamin D deficiency was significantly greater in patients with allergic rhinitis than the normal population (30% vs. 5.1%; p = 0.03) demonstrating that there is an association between serum vitamin D levels and allergic rhinitis status. While much larger studies are required to reconfirm our findings .These results may indicate subtle differences in terms of vitamin D metabolism or sensitivity in allergic patients, as hypothesized by Wjst et al. [15]
In conclusion as Bruce W. Hollis stated "The assessment of vitamin D is rapidly becoming an important tool in the diagnosis and management of many diverse pathologies" [16] therefore measuring serum levels of vitamin D could be considered in the routine assessment of patients with allergic rhinitis in Iran. Then vitamin D supplementation could be prescribed according to the status of deficiency. This could improve allergy symptoms directly or indirectly by potentiating the anti-inflammatory effects of the medications used to treat allergy as Searing et al. [17] have stated that there should be possibility of vitamin D effect on glucocorticoid pathway and vitamin D insufficiency promotes the needs for higher doses of glucocorticoids to achieve treatment effect. On the other hand recent studies suggest that vitamin D plays an important role in prevention of various allergic diseases, by activating certain regulatory immune cells that prevent release of chemicals that cause and worsen allergic disease; particularly allergic conditions have shown an association with mutations in vitamin D receptor genes [18]. Finally, large multi-center prospective studies are required to confirm our findings linking allergic rhinitis and lower serum levels of vitamin D. Then further research is required to adequately measure the potential benefit of vitamin D therapy in allergic conditions.

 XML Download
XML Download