

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Conventional endodontics relies on intraoral radiograph which can provide various information on the diagnosis of anatomical variations, the morphology and curvature of roots, configuration and number of root canals, and estimation of the preoperative canal length. Intraoral radiographs obtained at different beam angulations reveal various perspectives of multirooted teeth, but such two-dimensional imaging of three-dimensional (3D) anatomy is limited by superimposition and geometric distortion.1 Cone-beam computed tomography (CBCT) provides precise 3D images to facilitate diagnosis and treatment.2 However, endodontics requires a high level of image detail, and CBCT scans have lower spatial resolution than intraoral radiographs. CBCT may be justifiable where intraoral radiographs provide equivocal or inadequate information for treatment planning, as in the case of root canal system anomalies.1,2,3
The success of endodontic treatment depends partly on recognition of anatomic variations.4 For example, the pulp canal configuration of mandibular second premolars varies in about one-third of the population and may present as C-shaped canals.5,6 The reported incidence rate of two or more foramina in mandibular second premolars is 8.2%, whereas that in mandibular first premolars is 21.1%.5 Reports of three or more canals in mandibular second premolars are quite rare.7,8,9,10,11 Such anatomic variations have been investigated by micro-computed tomography (micro-CT). Micro-CT enables 3D assessment of the root canal system, but it can be used only in vitro.12,13
Here, we describe the endodontic treatment of a mandibular second premolar with aberrant pulp canal morphology detected by CBCT and confirmed by 3D modeling.
Case Report
A 21 year old woman was referred to the Faculty of Dentistry, Kocaeli University, Turkey, because of the pulsating pain in mandibular permanent left second premolar. The first premolar had been extracted. Intraoral examination revealed a carious lesion on the mesial and distal aspect of the tooth in proximity to the pulp chamber. The tooth was sensitive to percussion. Cold test revealed a strong and prolonged reaction. Periapical radiograph suggested abnormal root canal morphology dividing into multiple root canals with no periapical radiolucency (Figure 1a). The tooth was diagnosed as irreversible pulpitis, and endodontic treatment was initiated. Access was gained to the pulp chamber under rubber dam isolation, and all carious material was removed. Canal orifices were not easily located because of their apical positioning. Exploration with magnifying loupes (Heine HR Binocular Loupe, Heine Optotechnik, Herrsching, Germany) disclosed three pulp canal orifices. Intraoral radiographs taken at different angulations to evaluate working length suggested the presence of an accessory canal, and advanced imaging was performed. Informed consent was obtained from the patient.
CBCT (96 kVp, 12 mA, 5.5 cm-diameter field of view, and 5.0 cm-height, Planmeca ProMax 3D Max, Planmeca Oy, Helsinki, Finland) revealed a single pulp canal at the cervical third of the root. A high resolution (voxel size, 0.100 mm3) was used to investigate the cross-sectional morphology. After image acquisition, the CBCT images were subsequently reconstructed with Planmeca Romexis (Planmeca Oy). For 3D modeling, images were exported into the computer in DICOM format and were imported into MIMICS software (MIMICS version 12.1, Materialise, Leuven, Belgium). A thresholding process was performed to separate the tooth and its root canal from soft tissue. The manual editing tools (i.e., draw and erase functions) were used to restore the mask after the region-growing process. 3D reconstruction of the root surface and root canal configuration models were developed with a smoothing algorithm using 8 and 6 iterations and smoothing factors of 0.6 and 0.4, respectively.
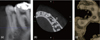
Axial cross-sectional images obtained with 1 mm interval demonstrated three canals in the middle third. One canal bifurcated in the apical third, and four foramina were identified (Figure 2). The root surface had a proximal lingual groove in the middle third. These findings suggested C-shaped canal morphology (Figure 3).14 3D modeling of the CBCT images confirmed an oval-shaped pulp canal in the cervical third and three branches in the middle third of the root. The mesiobuccal canal divided into buccal and lingual branches in the apical third of the root. The root was fused and had a deep lingual groove (Figure 4).
Working length was determined by periapical radiograph and verified with an electronic apex locator (Raypex 6, VDW GmbH, Munich, Germany) (Figure 1b). To gain sufficient access to the canals, the existing opening was enlarged with Gates-Glidden drills (sizes 1 - 3). The canals were cleaned and shaped with rotary files (ProTaper Universal, Dentsply Maillefer, Ballaigues, Switzerland). Obturation was performed by lateral compaction of gutta-percha and root canal sealer (AH Plus, Dentsply Maillefer) (Figure 1c). Twelve months postoperative clinical and radiographic examinations revealed that the tooth was asymptomatic and did not have periapical pathology (Figure 1d).
Discussion
Effective cleaning and disinfection as well as complete obturation of the root canal system are prerequisite for successful endodontic treatment.15 An operating microscope enhances visualization of canal orifices.16 Nevertheless, the lower two-thirds of the pulp canal is difficult to assess from the morphology of the cervical third in mandibular premolars with anomalous pulp canal configuration.14 Yu et al. reported a high probability of pulp canal variations in the middle or apical third of mandibular premolar roots and suggested that most mandibular premolars have an oval cross-sectional morphology in the cervical third.6 We identified a similar morphology. The pulp canal divided in the middle third and the orifice of the fourth canal could not be confirmed by exploration with magnifying loupes.
Relative root outline and shape must be carefully examined in periapical radiographs before endodontic management. Sudden narrowing of a pulp canal on a radiograph suggests the presence of multiple canals.17 CBCT can provide valuable information for assessing such complex morphology.16,18 However, its use in endodontics has been limited to selected cases in which intraoral radiographs were unsatisfactory for treatment planning.19,20 In the present study, CBCT revealed a fourth canal and 3D modeling of the tooth anatomy provided information about both the internal and the external morphology of the root, enabling preoperative evaluation and facilitating treatment.
Evaluation of anamolus root morphology with intraoral radiographs may suffer from the buccolingual superimposition. There may be a fused root with C-shaped canal configuration with seperate foramina, which may mimic seperate root canals in working length radiographs and postoperative radiographs after obturation. In this case, an additional root canal was suspected during the evaluation of working length radiographs and fusion of the root canals were revealed by CBCT.
Mandibular premolars tend to have anatomic variations with complex pulp canal morphology.7,8,11,21,22 The incidence of variations in the number of canals, roots, and foramina is lower for the mandibular second premolar than for the mandibular first premolar.23 Fan et al. classified C-shaped canals in mandibular first premolars and reported that the cross-sectional morphology of pulp canals may change from the orifice to the apex.14 The reported incidence rate of this anomaly in mandibular second premolars is 0.6%.6 In our patient, the isthmus and fused root morphology presented a C-shaped canal. To the best of our knowledge, this is the first report of a C-shaped canal with four separate foramina in a mandibular second premolar.



 XML Download
XML Download