

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Focal myositis, a benign inflammatory pseudotumor disease in skeletal muscle, was first reported in 1977 by Heffner et al.1). There have been assumed that viral infection, muscle denervation, autoimmunity, and family factors are related to the occurrence of the disease; however, it has not been clarified yet2). In the past, it was diagnosed as finding of inflammatory muscle disease such as lymphocyte infiltrate around muscle fiber from muscle biopsy. But recently, magnetic resonance imaging (MRI) is employed as a useful diagnostic method3). Focal myositis is known to occur mostly at lower extremity, but we could not find a report of occurrence around hip. Therefore, the authors attempt to report 3 cases of focal myositis that occurred around hip joint along with literature review.
CASE REPORT
1. Case 1
A 54-year-old woman visited an orthopedic outpatient clinic in the hospital with a chief complaint of the around right hip pain that occurred for non-specific traumatic cause from 5 days ago. The patient had no specific past medical history. The body temperature was 36.6℃, and other vital signs were within the normal ranges. She had no radiating pain toward lower extremity in a straight leg raising test. There was no muscular weakness in lower extremities.
Swelling and tenderness at posterolateral aspect of right hip were found from physical examination, and the patient complained of aggravated pain in hip joint motion. The results of peripheral blood examination were hemoglobin (Hb) 12.8 g/dL, white blood cell (WBC) 9,800/µL (normal, 4,000-10,800/µL), erythrocyte sedimentation rate (ESR) 5 mm/hr (0-9 mm/hr), C-reactive protein (CRP) 0.3 mg/dL (0-0.5 mg/dL), blood urea nitrogen (BUN)/creatine (Cr) 14.3/0.73 mg/dL, and aspartate aminotransferase (AST)/alanine aminotransferase (ALT) 26/22 IU/L. In addition, creatine phosphokinase (CPK) 78 IU/L (0-170 IU/L) and rheumatoid factor (RF) 3.6 IU/mL (0-14 IU/mL) were also normal.
No particular adverse result was not observed in the pelvic region plain radiograph. From T2 fat suppression image and T1 contrast enhanced fat suppression image in pelvis MRI, results of increased signal intensity and contrast enhancement were found on gluteus medius muscle, and there was intramuscular edema without subcutaneous edema, and increased muscle volume than contralateral normal side (Fig. 1A, B).
The patient was orally administered non-steroidal anti-inflammatory drugs (NSAIDs), and she left the hospital at day 6 of hospitalization because her symptoms were improved. In the follow-up observation conducted after 3 months, CRP was normal with 0.2 mg/dL (0-0.5 mg/dL), and even in MRI, abnormal signal intensity which was observed at gluteus medius was eliminated (Fig. 1C). There was no recurrence of the symptom in the follow-up result after 3 years and 6 months.
2. Case 2
A 63-year-old female patient visited hospital for pain in right around hip that occurred without particular injury. The patient was transferred after conducting spine MRI at outpatient spinal department. In the spine MRI, there was no lesion that explained the cause of the pain of the patient (Fig. 2A). The patient had no special past medical history except for high blood pressure. The body temperature was 36.7℃, and other vital signs were within normal ranges. She had severe swelling and tenderness at posterolateral aspect of right hip in physical examination and the patient complained of serious pain in joint motion.
The peripheral blood examination showed that Hb 10.5 g/dL, WBC 5,700/µL, ESR 16 mm/hr and CRP 0.2 mg/dL, AST/ALT 17/15 IU/L, BUN/Cr 21.5/0.63 mg/dL, uric acid 2.95 mg/dL (2.6-7.2 mg/dL), RF (1.5 IU/mL), anti streptolysin O 22.55 IU/mL (0-200 IU/mL) and CPK 65 IU.
In the pelvis MRI, T2 fat suppression image and T1 fat-suppressed contrast enhancement image showed results of increased signal intensity and enhancement in gluteus medius and gluteus minimus (Fig. 2B, C). The symptom of the patient was improved after administering NSAID. She was discharged after 10 days of the hospitalization, and no recurrence of symptoms was observed at the 2-year follow-up.
3. Case 3
A 50-year-old female patient visited hospital as an outpatient for pain in left hip joint that occurred 3 days before hospitalizing without particular trauma history as a chief complain. The patient had no special past medical history, and her body temperature was 37.7℃ with a fever, and other vital signs were of normal ranges. She complained of tenderness and pain at the front portion of inguinal region in hip joint motion. No decreased muscular strength was found in physical examination.
Peripheral blood test showed Hb 12.7 g/dL, WBC 7,600/µL, ESR 6 mm/hr, CRP 0.7 mg/dL and CPK 100 IU/L at admission. In the next day, her CRP was even more increased to 4.7. Because the patient was accompanied by a fever, autoimmune antibody test was conducted for differential diagnosis. RFs were found to be 5.9 (0-14 IU/mL), ANA (-), anti-DNA (-), anti-Jo-1 antibody (-), anticetromere antibody (-), and HLA-B27 (-). Complement C3 and C4 were within normal ranges.
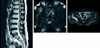
Signal intensity was increased in left iliopsoas muscle on T2 fat suppression MRI, and in T2 Fat suppression with contrast enhancement, there was contrast enhancement on left iliacus muscle (Fig. 3A, B). We considered that there was a possibility of abscess, but MRI finding showed myositis without abscess.
The body temperature of the patient was restored to normal range after the 2nd day of the hospitalization, but her pain was not much improved through NSAID. Since the 10th hospital day, methylprednisolone 40 mg was administered through intravenous injection. The pain of the patient w as gradually subsided and CRP was decreased to 0.5 after 2 days of the steroid injection. The authors conducted an electromyogram (EMG) to differentiate from polymyositis because the response of patient was weak to NSAID and high fever. In the conducted electromyography, abnormal results for iliopsoas muscle were not showed.
At the 12th day of hospitalization, she showed improvement of clinical symptom and CRP returned to normal range, and then discharged from the hospital. There was no outpatient follow-up after discharge from hospital, but it was found that she was fine without recurrence of the symptoms through the telephone interview which was conducted after 1 year and 6 months.
DISCUSSION
Focal myositis, the disease occurring as benign inflammatory pseudotumor disease in skeletal muscle, has been mostly reported in thigh in lower extremity, or rarely reported in hands, neck, or tongue2,3,4). The authors have not found case reports that occurred in muscles around hip joint because it is thought that the muscle around hip joint as like iliopsoas muscle is located at a deep, so it does not create a shape like tumor superficially despite the occurrence of inflammatory edema, compared to other parts of body, and because progression of the disease is spontaneously cured with anti-inflammatory drug, so it will be able to misdiagnosed as spinal stenosis, rheumatoid disease, abscess and calcific tendinitis without accurate additional examinations that are needed for diagnosis.
Because polymyositis, the typical disease among inflammatory myopathy, starts from the pain in pelvic girdle muscle to gradually progression to more distal muscle with decreased muscular strength, the differentiation for hip pain is needed. Focal myositis does not generally involve fever, weight loss, and decreased muscular strength, and in blood test, most muscle enzymes such as lactate dehydrogenase, and CK are normal despite the fact that it is muscular disease. On the other hand, in the beginning of polymyositis, fever, weight loss, decreased muscular strength as well as increases of ESR and CRP are entailed. Also, because there are reports that focal myositis is likely to develop polymyositis when CPK and ESR are increased, careful observation is needed here5,6).
Focal myositis shows inflammatory cell infiltration in biopsy, but it's difficult to differentiate it from other inflammatory muscular diseases only through histological results3). When considering progress and treatment of the disease, it is thought that instead of conducting biopsy at first, it is useful to differentiate it from tumor through MRI and then diagnose myositis. In addition, it is helpful for diagnosis to observe that clinical progression is generally improved by NSAID.
Heffner et al.1) reported 6 cases that myositis progress polymyositis, and ESR was reported to increase in those cases. For case report 3, the patient had a fever of 37.7℃ from her visit to hospital, and CRP was increased to 0.7. Also, because the fever was continued next day, and CRP was even more increased to 4.7, differentiations for recurrence type of infective myositis, focal myositis, autoimmune myositis, and especially polymyositis were needed7,8). Because autoantibody and EMG was negative, and the point occurring in unilateral side and muscle enzymes were normal, it was diagnosed as focal myositis rather than polymyositis. There was no outpatient follow-up, but it was found that the patient had no recurrence of symptoms for 1 year and 6 months from the recent follow-up telephone interview. However, because focal myositis may develop recurrent type and polymyositis when fever and increased ESR are involved, constant observation is needed9).
As for treatment, it is spontaneously improved after administering NSAID, but as shown in case 3, steroid may be used if improvement of symptoms is not observed quickly through NSAID and pain killer10). However, steroid is the primary selection drug for polymyositis, but attention is needed for focal myositis because the injection of steroid in the beginning may give confusion in differentiating the two diseases.
The authors report 3 cases of focal myositis around hip joint which is clinically rare, and when considering this disease in clinical medicine, it is thought that they will be help in avoiding unnecessary examinations or treatment.


 XML Download
XML Download