

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The majority of ingested foreign bodies (IFBs) are excreted though the digestive tract without complication or morbidity. However, they occasionally lead to serious clinical problems such as obstruction, perforation, or bleeding.1,2 Symptoms, should they occur, tend to manifest as an abscess or foreign body as the condition progresses. In adults, IFBS are usually ingested accidentally through food, and are detected in individuals exhibiting certain pathological changes of the gastrointestinal tract. Treatment for IFBs is common in clinical practice. A distinction is made between accidental ingestion and intentional ingestion with secondary gain. According to available data, types of swallowed foreign bodies vary widely. Those most commonly swallowed by adults are fish bones (9%~45%), other bones (8%~40%), and dentures (4%~18%).3,4,5 IFBs such as chicken bones, fish bones, toothpicks, and dentures, rarely require surgical intervention (5%). In fact, most patients are unaware of these IFBs, which are usually detected incidentally during laparotomy or pathological examination of surgical specimens.6 Foreign bodies pass naturally in 80% of cases, but in 20% of cases, endoscopic intervention is indicated. Surgical intervention is indicated in <1% of cases.3,4,5,6,7 Some cases of esophageal or gastrointestinal tract perforation due to IFBs have been reported, but gastric pseudotumoral lesions caused by fish bones are rare and have not been cited in the literature to date. Here, we report the case of a 59-year-old healthy woman who presented with a gastric pseudotumoral lesion mimicking a gastric submucosal tumor.
Case Report
A 59-year-old woman presented with a diagnosis of a gastric submucosal tumor detected incidentally during routine health screening. She had no known family history of gastrointestinal disorders or cancers. On admission, she had no symptom, including abdominal discomfort. Physical examination on admission revealed no abnormalities, and initial biochemical and hematologic test results for complete blood count, electrolyte levels, and liver function were all normal. Chest radiography revealed no abnormality, but gastroscopic examination revealed a bulging mucosa on the posterior wall of the gastric antrum (Fig. 1).
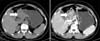
Non-contrast and contrast-enhanced abdominal computed tomography (CT) revealed a well-defined heterogeneous enhancing mass, approximately 3 cm in size, on the posterior wall of the gastric antrum (Fig. 2), suggestive of a submucosal tumor such as gastrointestinal stromal tumor, schwannoma, or leiomyoma. No evidence of distant metastasis or significant lymph node enlargement was noted. Laparoscopic surgery showed that the mass was not present on the posterior wall of the gastric antrum but adhered to the pancreas. After adhesiolysis, we incidentally found and biopsied the pancreatic mass-like lesion. Frozen section indicated the absence of a pathologic lesion. The gastric wall appeared to be intact with no tumor invasion, deformity, or evidence of a gastric submucosal lesion. However, on squeezing the gastric wall, the serosa of the adherent posterior wall was found to be torn. A foreign body protruding from the tear was found to be a 2.5×0.2-cm fish bone (Fig. 3). The procedure was completed with the suturing of the injured serosa with 2 stitches. These findings indicate that the mass-like lesion was a gastric pseudotumoral lesion caused by the impacted fish bone. The patient's post-operative course was uneventful.
Discussion
Sometimes a hepatic hemangioma, accessory spleen, or pancreatic pseudocyst can mimic a submucosal tumor of the stomach. Abdominal CT may show extrinsic compression of the stomach. Ingestion of foreign bodies is not uncommon, and fish bones are the most common IFBs, although most pass uneventfully through the gastrointestinal tract.1,2 Foreign body ingestion generally occurs in childhood but may occur in adults. In adults, IFBs are most commonly encountered in individuals with an alcohol or drug addiction, elderly individuals with dentures, prisoners, individuals with mental disorders or learning difficulties, fast eaters, or workers such as carpenters and dressmakers who tend to hold small sharp objects in their mouths.8,9 Elderly individuals may have trouble using dentures and are more prone to foreign body ingestion because of decreased feeling in the palate. Generally, patients are unaware of foreign body ingestion, and the objects are incidentally detected during radiological imaging, surgery, or pathological examination of surgical specimens.6
Symptoms, should they occur, tend to manifest later as abscesses. Serum amylase levels and liver function are generally within normal limits3,6,8 or occasionally elevated.8 However, all inflammatory response markers are nonspecific and, therefore, unreliable. Our patient had no abnormal biochemical and hematologic examination results.
Perforation of the gastrointestinal tract due to fish bone ingestion is rare.4,7,9 In fact, <1% of all IFB patients develop perforation.9 Our patient experienced epigastric discomfort that was assumed to be symptom of an enlarging abscess.
Gastric perforations by fish bones have been described previously. Goh et al.7 described a case in which a fish bone perforated the posterior stomach wall and migrated into the pancreatic body where it caused a pancreatic abscess. More recently, Bajwa et al. described a similar case of a gastric submucosal tumor; their patient eventually underwent elective distal gastrectomy for a suspected malignant mass.4
Our patient presented with an apparent gastric submucosal tumor on the posterior wall of the antrum, and thus, we performed laparoscopic surgery. However, the mass-like lesion was eventually identified as a gastric pseudotumoral lesion caused by a fish bone.
When perforating foreign bodies are identified early, that is, in the absence of symptoms of peritonitis, endoscopic retrieval may be possible. However, the preoperative diagnosis of a foreign body may be difficult. In particular, plain radiography of fish bones has a sensitivity of only 32% depending on the size and species; radiography is more sensitive in detecting chicken bones due to their higher density.4,9,10 Chicken bones are almost always radiopaque,8 whereas fish bones, even when radiopaque, may be obscured by large soft-tissue masses or fluid, particularly in altered or obese patients.9 In our case, the fish bone was not visible on plain abdominal radiograph, even retrospectively. CT has been shown to be beneficial in diagnosis when a linear calcified lesion is present4,7,9 and has a reported sensitivity of 71.4%, which increases to 100% for retrospective analyses.9 In our case, the fish bone was not visible on plain abdominal radiography, but the lesion was seen retrospectively on CT.


 XML Download
XML Download