

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Adenocarcinomas usually originate from the gastrointestinal tract, prostate gland, or other glandular tissues of the body. Metastasis from gastric adenocarcinoma typically occurs in the regional lymph nodes, liver, peritoneum, omentum, lungs, and mesentery. Metastasis to the prostate gland is very rare and most commonly occurs owing to direct invasion from neighboring organs or infiltration, in cases of hematological malignancies. Metastasis of gastric adenocarcinoma to the prostate gland is extremely rare. Herein, we report one such rare case.
Case Report
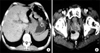
A 56-year-old man presented with dysphagia and diffuse abdominal pain lasting for 1 year. He had experienced symptomatic progression over the previous 6 months. Results of general and systemic examinations were normal, except for the presence of a perirectal growth on the anterior rectal wall, inseparable from the prostate gland. Computed tomography (CT) of the abdomen and pelvis revealed mural wall thickening, measuring 3.3×3.3 cm, involving the gastroesophageal junction and extending to the lesser curvature of the stomach as well as a prostatic mass (Fig. 1). CT of the neck and chest revealed no metastasis to other organs.
Upper gastrointestinal endoscopy revealed an ulceroinfiltrative growth at the gastroesophageal junction along the lesser curvature of the stomach (Fig. 2A), and a biopsy specimen was taken. Histopathological analysis showed gastric mucosa with ulceration and an infiltrative neoplasm composed of cells arranged in a glandular pattern, signet ring cells, and pools of mucin. These findings were consistent with moderate-to-poorly differentiated adenocarcinoma (Fig. 2B). The level of serum carcinoembryonic antigen was 2 ng/ml, and that of serum prostate-specific antigen (PSA) was 1.94 ng/ml, within the normal range.
To evaluate the prostatic mass, flexible sigmoidoscopy was performed, which revealed a sessile polyp in the rectum and enlargement of the prostate gland; biopsy specimens were taken. The biopsy specimen from the sessile polyp showed colonic mucosa with the lamina propria showing lymphoplasmacytic cells and eosinophils. Tru-cut biopsy of the specimen from the prostate gland showed infiltration of the small and large glands lined by tall columnar/cuboidal mucinous cells (Fig. 3A). Immunohistochemistry revealed positive staining for cytokeratin 7 and negative staining for PSA (Fig. 3B, C).
Thus, we confirmed the diagnosis of prostatic metastasis from a carcinoma of the stomach. The patient was treated with palliative chemotherapy consisting of epirubicin, oxaliplatin, and capecitabine; however, the patient was lost to follow-up after 3 courses of chemotherapy.
Discussion
Patients with gastric carcinoma most commonly show metastasis to the regional lymph nodes, liver, peritoneum, omentum, lungs, and mesentery. Metastasis of gastric adenocarcinoma to the prostate gland is extremely rare, and only a few cases have been documented in the literature.1,2 Secondary prostatic neoplasms usually arise due to direct invasion from adjacent tumors or infiltration, in cases of hematological malignancies such as leukemia or lymphoma.
True metastasis to the prostate gland from solid tumors is reported only in 0.2% of all surgical prostatic specimens and in 2.9% of all post-mortem analyses in men.3
Most secondary tumors in the prostate gland arise via direct spread, from either the bladder or the rectum. Direct spread from bladder carcinoma is the most common etiology of secondary prostatic tumors. Metastasis from nonadjacent organs is often diagnosed during autopsies; it primarily arises from cancers of the lung, skin (melanoma), gastrointestinal tract, kidney, bladder, and testes. Colorectal tumors including colorectal adenocarcinoma and gastrointestinal stromal tumor may also occasionally metastasize the prostate gland.
The lung is the most common primary site in cases of metastasis to the prostate gland. Bates and Baithun reported that, in a series of 17 prostatic metastases, the lungs and pancreas were the sites of the primary lesions in 8 and 2 cases, respectively.3
The most common presentations of secondary neoplasms of the prostate gland are prostatism, pelvic pain, and hematuria; patients with secondary neoplasms of the prostate gland are usually symptomatic, particularly those with widely disseminated disease. Occasionally, these symptoms mimic those of a primary prostatic cancer.
Analysis of the clinical and radiological features, pathological characteristics, and immunohistochemical localization of PSA is helpful in differentiating between primary and secondary tumors of the prostate gland.
The mechanism of spread from the stomach to the prostate gland is not clear. The prognosis and therapy of patients with metastatic adenocarcinoma are often linked to the site of origin; these patients are usually investigated with clinical examination, radiological analysis, and evaluation of the levels of serum tumor markers.
Primary adenocarcinoma of the prostate gland can be differentiated from secondary tumors involving the prostate gland by using immunohistochemistry. Among prostatic markers with the greatest specificity for the prostate gland, the most sensitive are PSA, prostein (P501S), and Nkx3.1. Immunohistochemical staining for PSA is diagnostically helpful in distinguishing between prostatic adenocarcinomas and other neoplasms that secondarily involve the prostate gland. It is also useful in establishing a prostatic origin in cases of metastatic carcinoma with an unknown primary site.4 PSA, however, is not entirely specific for prostatic adenocarcinoma as its expression has also been detected in carcinomas of the ovary and the breast, including in male breast cancer, but it is still the most commonly used prostate cancer marker. P501S is used to distinguish a tumor of prostatic origin from those of the colon and bladder. It is still regarded to be among the best-validated immunohistochemical markers for tumors of prostatic origin. Nkx3.1 is another sensitive and specific prostate cancer marker.
The prognosis of prostatic metastasis is very poor, as secondary tumors usually occur in patients with late-stage carcinoma.


 XML Download
XML Download