

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Question: A 52-year-old woman visited our hospital complaining of lower abdominal pain and intermittent chilly sensations for three weeks. She had taken over-the-counter remedies for a cold three weeks prior to her visit. As the symptoms persisted, she visited another clinic where she underwent an esophagogastroduodenoscopy and colonoscopy. The esophagogastroduodenoscopy did not reveal any possible cause of her abdominal pain. Colonoscopy revealed a long and thin foreign body perforating her sigmoid colon, and this led to her being admitted to the outpatient clinic of our hospital.
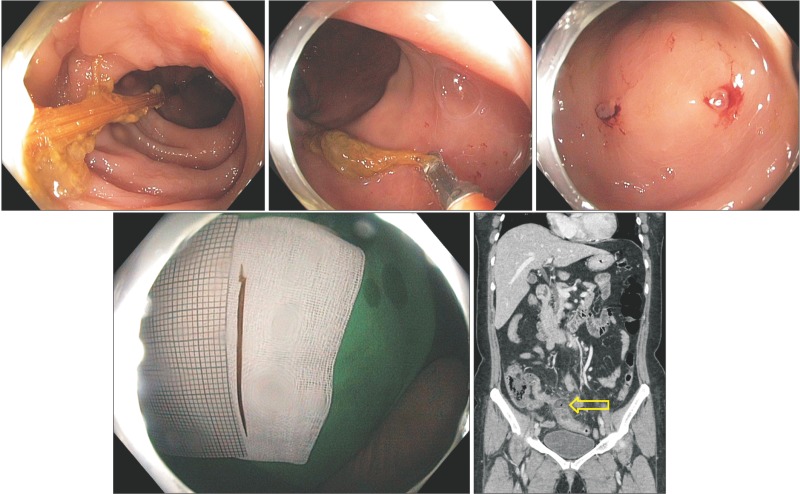
Her medical history involved no serious illness or surgical procedure besides hypertension. We performed a sigmoidoscopy to evaluate and remove the foreign body. This revealed a hard, long, and thin foreign body lodged in the sigmoid colon, with both ends impacted into the bowel wall (Fig. A). The end of the foreign body was carefully and firmly grasped with forceps, and gently dislodged from the colon wall (Fig. B). It was easily removed intact through the anus, and the procedure was uneventful. Focal mucosal edema with bloody erythema was noted at the sigmoid colon after removing the foreign body (Fig. C). Her abdominal pain improved considerably immediately after removal.
The post-procedure abdominal radiograph was negative for pneumoperitoneum. An abdominal CT scan was performed, and revealed a small amount of extraluminal air with surrounding fluid at the sigmoid mesocolon, and short-segmental sigmoid colon edema. Treatment with intravenous broad-spectrum antibiotics was initiated while she remained fasted. A regular diet was introduced gradually after five days of fasting. During this period, she noted complete resolution of her lower abdominal pain and chilly sensations. What is the most likely diagnosis?
Answer to the Images: A Toothpick Perforating the Sigmoid Colon
The ingestion of foreign bodies is a common clinical problem. Large, thin, and sharp objects (toothpicks, chicken or fish bones, and metal objects) carry a high risk of bowel perforation.1 Swallowed objects larger than 65 mm in length that pass beyond the esophagogastric junction are likely to cause complications and require surgical intervention.2 Toothpick ingestion is commonly implicated in bowel injuries due the two sharply pointed ends and indigestible hard body of the object, which make it difficult for the toothpick to pass the intestinal lumen, especially in the narrow or tortuous sections of the gastrointestinal tract or at the transition from a mobile portion of the bowel (ileum and sigmoid colon) to a more fixed portion (cecum and rectum).3
In this case, a healthy woman presented with intermittent lower abdominal pain that started a few days after the accidental ingestion of a toothpick. She had no psychiatric problems, normal teeth, and had not been drinking alcohol at the time. After she was informed that the foreign body was a toothpick (Fig. D), she remembered eating with the aid of a toothpick three weeks prior. However, she did not experience any symptoms while swallowing the toothpick, nor did she recall ingesting it.
After removing the toothpick, an abdominal CT scan revealed microperforation at the sigmoid colon (Fig. E). Her symptoms were improved by conservative treatment over several days. Intestinal perforation due to foreign body ingestion should be considered in the differential diagnosis of patients presenting with abdominal discomfort or abdominal pain, even when they do not recall any foreign body ingestion.4
 XML Download
XML Download