

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
고혈압은 다양한 병인을 가진 질환이다. 젊어서는 교감 신경계 또는 레닌-안지오텐신계 활성이 고혈압 발생의 주기전이고, 그리고 나이가 들어서는 소금 및 볼륨증가가 혈압상승을 이끄는 주 기전이다. 60여 년 전부터 고혈압 약제의 개발도 이런 기전에 따라서 베타차단제, 알파차단제, 알파-베타차단제와 같은 교감신경억제제, 체내 소금 및 볼륨을 줄이기 위해 이뇨제와 칼슘채널차단제가 개발되었고, 안지오텐신수용체차단제 또는 안지오텐신전환효소 억제제와 같은 레닌-안지오텐신계 활성억제제가 개발되어 성공적으로 사용하고 있고, 최근에는 직접 레닌억제제, 알도스테론 길항제 등이 고혈압 약물로 소개되었다. 최근에는 우리나라를 비롯하여 여러 나라 고혈압진료지침에서는 중요한 약물계통을 A (angiotensin receptor blocker, angiotensin converting enzyme inhibitor), B (beta-blocker), C (calcium channel blocker), D (diuretics) 4가지로 분류하여 고혈압 치료의 첫 번째 약물로 추천하고 있다[1]. 하지만 고혈압환자가 첫 번째 추천하는 약물에 반응하거나 조절되는 경우는 1/3 정도 밖에 되지 않아서 많은 환자들이 약의 용량을 올리거나 아니면 다른 약을 추가로 필요로 하게 된다[234]. 약의 효과 면이나 부작용감소 측면에서는 약의 용량을 올리는 것 보다는 다른 약을 추가하는 것이 더 효과적인 것으로 알려져 있다[56]. 그 다음은 어떻게 약을 배합할 것인가이다. 첫 번째 약의 용량을 올리거나[5], 같은 기전을 가진 고혈압을 배합하는 것[7] 보다는 서로 기전이 다른 두 가지 고혈압 약을 배합하는 것이 효과나 부작용 면에 있어서 우위에 있다고 알려져 있다.
고혈압 기전과 고혈압 약물
혈압은 신경 체액성 요소, 대사적인 요소, 혈역학적인 요소가 함께 작용하여 결정된다. 고혈압의 발생은 유전적 요소와 스트레스, 소금, 비만 등의 환경적 요소가 서로 상호작용을 하여 초기에는 볼륨 증가에 의한 심박출량의 증가, 교감신경 항진에 의해 혈압이 상승하기 시작하고 이는 말초혈관의 재형성과 수축력 증가에 따라 말초저항의 증가가 일어나서 혈압이 상승한다(Figure 1). 젊을 때는 심박출량이 정상 혹은 약간 증가에 의해 혈압이 상승하나(이때 말초저항은 정상이다), 약 20년 경과 후에 서서히 심박출량은 점진적으로 정상으로 되고 말초저항이 증가하여 혈압을 상승시키고 고혈압을 유지 악화시킨다. 성인에서 나타나는 고혈압은 말초저항 증가에 의한 확장기혈압 상승에 의해 나타나고, 나이가 더 들어가면서 중심동맥(대동맥, 경동맥 등)의 섬유화, 석회화 등에 의해 혈관이 딱딱해지고 이는 심장 → 중심동맥 → 혈관분지 및 말초혈관으로 진행되는 맥파형이 일찍 중심동맥으로 되돌아와서 증폭되어 수축기고혈압으로 발전하게 된다. 따라서 고혈압 약물의 개발도 기전에 대한 이해와 같은 맥락에서 초기에는 볼륨감소를 위해서 이뇨제, 교감신경항진 억제를 위해 베타차단제, 알파차단제, 알파-베타차단제가 개발되었고, 이후에 말초혈관저항을 줄이기 위해 칼슘통로차단제 및 말초혈관저항에 중요한 역할을 하는 레닌-안지오텐신계 억제제(안지오텐신 전환효소억제제 및 안지오텐신수용체차단제)가 개발되어 이들이 지금의 고혈압 약물치료의 근간을 이룬다. 이런 기전을 바탕으로 더 발전된 형태의 약이 개발되는데, 예로, 베타차단제는 교감신경을 감소시켜서 심박수 감소 및 수축력을 떨어뜨려 혈압을 떨어뜨리지만 혈관수축을 일으키고 대사합병증을 증가시키는 단점이 있는데 nebivolol과 bisoprolol은 베타-1 선택성을 증가시키고 nebivolol과 carvedilol은 일산화질소(nitric oxide)의 생체이용률을 증가시켜 혈관을 확장시키고 대사장애가 비교적 적은 3세대 베타차단제가 개발되었다[8]. 또 레닌-안지오텐신계 차단을 위해 안지오텐신전환효소억제제, 안지오텐신-1 수용체차단제 순으로 개발되었지만 이후 이 시스템의 가장 첫 단계인 레닌을 직접 억제하는 레닌억제제가 개발되었고, 마지막 단계에 있는 알도스테론길항제도 저항성고혈압 등에서 항고혈압약으로 사용되고 있다.
고혈압 약물 병합요법의 시작
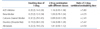
고혈압 환자의 약 2/3 이상에서는 한가지 종류의 약으로 조절되지 않으며, 그 이유는 고혈압의 발생기전이 다양하기도 하고 또 환자가 성인이 되어 고혈압이 나타나면 고혈압 발생이 한가지 보다는 여러 가지 기전이 섞여서 발생하기 때문에 하나만 조절한다고 혈압이 떨어지지 않고 또 하나를 억제하면 반대로 다른 하나가 활성화되기 때문에 한가지 고혈압 약으로는 조절이 잘 되지 않는다[3]. 그래서 첫 번째 고혈압 약으로 조절되지 않으면 기전이 서로 다른 2가지 이상의 강압제가 필요하다. 고혈압의 혈압 정도가 크지 않거나 단순 고혈압인 저·중등도 위험 고혈압인 경우에는 한가지 약으로 시작할 수 있다. 처음 사용한 일차약에 효과가 없을 때는 다른 약으로 교체하고, 약간의 효과는 있으나 목표혈압에 도달하지 못하면 용량을 증가시키거나 다른 기전의 약을 추가한다. 그러나 용량을 늘리기보다는 서로 작용이 다른 약을 소량씩 추가하는 것이 더 혈압 강하에 효과적이다. 42개의 임상연구에서 11,000명을 대상으로 한 메타분석에서는 한 가지 약제의 용량을 두 배로 증량했을 때 실제 추가로 하강한 혈압의 크기가 예측한 추가 혈압 하강의 정도에 비해 약 5분의 1 정도 밖에 되지 않은 반면, 작용 기전이 다른 약제를 추가한 경우는 예상한 추가 혈압 하강의 정도만큼 혈압이 하강하였다(Table 1) [5]. 또한 소량 병합요법이 부작용도 적기 때문에 환자의 순응도도 더 높다. 2기 이상 고혈압(160/100 mmHg) 중에 혈압 정도가 높거나, 고위험 고혈압 또는 목표혈압이 낮은 환자에서는 처음부터 다른 기전의 고혈압약을 저용량 병합할 수 있다(Figure 2).
단일 약으로 혈압이 조절되지 않으면 그 다음에는 어떻게 약을 배합할 것인가가 중요하다. 어떤 형태로든지 기전이 다른 두 가지 고혈압 약물로 치료하는 것은 단일 약 용량을 증가하는 것보다 혈압 강하효과가 우수하기 때문에 기본적으로는 모든 종류의 배합이 가능하다. 하지만 같은 계통의 고혈압 약을 복합하는 것은 권하지 않는다. 예로 안지오텐신전환효소억제제와 안지오텐신수용체차단제는 두 약을 같이 복용하면 혈압 강하효과가 크고 단백뇨 감소효과도 크지만 저혈압의 위험이 커져 심혈관질환 예방효과가 더 좋아지지는 않기 때문에 권하지 않는다. 어떻게 복합하는 것이 더 좋은 가에 대한 장기적 임상연구는 아직 매우 부족하지만, 대부분의 나라에서는 레닌-안지오텐신계억제제, 칼슘길항제, 이뇨제 3가지 약을 가지고 약물 복합하도록 하고 있다.
병합요법 방법
2011년 영국고혈압진료지침(National Institute for Health and Clinical Excellence, NICE 지침) [9] 2013년 유럽가이드라인(European Society of Hypertension and of the European Society of Cardiology, ESH/ESC) [10], 제8차 미국 통합 진료지침 가이드라인위원회(Joint National Committee, JNC 8) [11], 미국고혈압학회·국제고혈압학회 통합 가이드라인(American Society of Hypertension-International Society of Hypertension, ASH-ISH) [12] 및 우리나라 대한고혈압학회 가이드라인이 발표되었다[1]. 이들 각 대륙별, 나라별 약 병합요법에 대해서는 약간씩 달리하고 있지만 대부분은 기조는 비슷하다. NICE 지침은 A 계통약물+C 계통약물을 우선 권하고 다음 A+C+D 병합, 그 이후에는 A+C+D+기타 약물(다른 이뇨제, 베타차단제, 알데스테론차단제 등)을 복합하도록 하고 있다. 반면 유럽은 초기약물로 A, B, C, D 약물 모두 가능하고 첫 번째 약으로 조절되지 않으면 A, C, D 중 두 가지를 가지고 우선 병합하고 조절되지 않으면 세 가지 약물을 병합하고 그래도 조절되지 않으면 NICE 진료지침처럼 기타 약을 추가하도록 하고 있다. 우리나라 고혈압 진료지침에서도 이와 비슷하게 일차약으로 A, B, C, D 약물을 모두 자유롭게 사용할 수 있도록 하였고, 조절되지 않으면 A, C, D 세 가지 약 중에 A+D, 또는 A+C 병합하도록 하였고, 이로써 조절 안되면 A+C+D를 병합하도록 하였다. B+D 도 사용 가능한 병합이긴 하지만 당뇨병 등의 대사적 장애를 다른 약의 병합보다는 더 발생할 수 있기 때문에 조심해서 사용하여야 한다(Figure 3). 임상연구를 토대로 A+C 또는 A+D 배합을 먼저 권하고 이외에 다른 배합도 환자의 특성에 따라 사용할 수 있다(Table 2) [1314151617181920].
병합요법 그 이후
일반적으로 고혈압 병합요법은 A, (B), C, D 네 가지 일차약을 기본 틀로 하여 3가지 약을 병합한다. 이뇨제를 포함하여 작용기전이 다른 강압제를 3가지 이상을 최대한 사용하여 병합 투여함에도 불구하고 혈압이 140/90 mmHg 이하로 조절되지 않는 경우(저항성 고혈압), 그 다음은 어떻게 할 것인가이다. 국내 자료는 없으나 외국에서는 치료 중인 환자의 저항성고혈압의 유병률은 5-30%로 보고되었고 실제로는 10% 미만일 것으로 추측한다. 이들 고혈압환자에서 심혈관질환과 콩팥질환 합병증의 발생 위험이 높다. 이런 경우에, 고혈압 약의 실제 복용여부 확인을 비롯하여 24시간활동혈압 측정하여 백의성효과(병원 이외에서는 혈압이 높지 않지만, 병원에서 측정하면 혈압이 올라가는 효과)가 큰 것은 아닌지 또 백의성고혈압은 아닌지, 이차성고혈압 여부 등을 확인하여야 한다. 혈압이 실제로 높으면 다른 기전의 네 번째 고혈압 약물을 추가하며 spironolactone 또는 doxazosin과 같은 알파차단제를 추가한다[2122]. 약으로 조절되지 않는 경우 최근에 소개되고 있는 관혈적 고혈압 치료법을 이용할 수 있다. 그 중 양쪽 콩팥동맥의 신경을 카테터를 이용하여 절단하는 시술인 콩팥교감신경차단술이 주목받고 있으며[23] 시술 후 혈압 감소효과가 3년 추적관찰에서도 그 혈압 감소효과가 유지되는 것으로 보고되고 있으나 최근에는 반대의 결과들도 발표하고 있어서 좀 더 연구결과를 지켜봐야 하겠다. 현 단계에서는 고혈압 병합요법으로 조절되지 않는 고혈압환자에서 적극 권장하기는 어렵다.
결론
대부분의 고혈압환자가 한가지 고혈압 약에는 반응하기 않기 때문에 두 가지 이상 약의 병합요법이 필요하다. 첫 치료약인 A군 약물인 레닌-안지오텐신억제제, C군 약물인 칼슘차단제, D군 약물인 이뇨제, B군 약물인 베타차단제(북미, 국제고혈압학회에서는 일차약에서 제외됨)를 가지고 병합하는데 주로 A, B, C군 계통약으로 먼저 병용 치료한다. 이 세 가지 병합 약물치료에도 불구하고 혈압이 조절되지 않는 고혈압이 10% 정도 될 것으로 생각되고 이 경우에는 베타차단제 또는 다른 약을 병합하여 조절한다. 약으로 조절되지 않는 진성 저항성고혈압인 경우에 관헐적시술을 이용하여 혈압을 조절 할 수 있겠다.
Peer Reviewers' Commentary
고혈압의 적절한 관리는 심혈관질환의 예방을 위한 중요한 수단이다. 우리 나라 고혈압 관리 현황은 과거에 비해 괄목할 정도로 개선되었으나 고혈압 환자 가운데 혈압이 목표 수준에 도달해 있는 경우가 아직도 50%에 이르지 못하고 있다. 고혈압 환자들에서 이렇게 혈압의 관리가 적절하지 못한 것은 고혈압 약제의 효과가 충분하지 못한 문제, 환자의 순응도 문제 및 고혈압 약제를 처방하고 관리하는 의사들의 관성(inertia) 등 여러 가지가 거론되고 있으며, 이들이 복합적으로 작용할 것이다. 고혈압 약제의 효과가 적절한지의 관점에서 보면 지금까지 여러 다양한 기전을 가진 고혈압 약제들이 개발되었지만 한 가지 고혈압 약제의 혈압 하강 효과는 상당히 제한적이어서 고혈압을 목표 혈압으로 조절하려면 2개 이상의 다른 기전을 가진 고혈압 약제를 함께 사용하여야 하는 경우가 대부분이다. 이 의학 강좌에서는 실제로 어떤 고혈압 약제를 어떻게 병용하는지에 대해 고혈압 약제들의 작용기전의 설명과 함께 자세히 기술하고 있으며, 특히 최근에 발표된 여러 나라의 고혈압 관리 지침들을 비교하여 소개하고 있어서 실제 임상에서의 활용성이 높다고 생각된다.
[정리: 편집위원회]




 XML Download
XML Download