

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Holoprosencephaly is a birth defect that occurs during the first few weeks of intrauterine life. Holoprosencephaly is characterized by a failure of transformation of the prosencephalon into cerebral hemispheres with separate lateral ventricles [1]. Holoprosencephaly has many associated anomalies, both of the nervous system and face [2].
In all described types of holoprosencephaly and recently reported variational forms, cerebral ventricles that ranging from a single ventricle (monoventricle or holoventricle) to relatively normal ventricles are present [345].
A new variant of holoprosencephaly has been reported recently where there is an absence of the ventricles and is termed as aventriculi [678]. To our knowledge, only three holoprosencephaly cases with aventriculi have been reported in the literature [678]. Here, we presented a case demonstrating aventriculi associated with holoprosencephaly.
Case Report
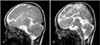
A 6-month-old boy suffering from motor and mental retardation was referred to our university hospital for further investigation. He was born after an uncomplicated and a full term pregnancy. Birth weight was 3,250 g, but there was no data about head circumference at birth. Family history was unremarkable; the parents were fourth degree consanguineous. On admission, weight and height values (8,000 g and 68 cm, respectively) were at the normal percentile. His head circumference was 40 cm (<3rd percentile). His head control was poor and he was not able to sit with support. He was hypertonic and deep tendon reflexes were hyperactive. He was conscious, but he was not able to follow visual and aural stimuli. Other neurologic and systemic examinations were normal. In laboratory examination, complete blood count, serum biochemical and urine analysis, thyroid functions were within normal limits. Abdominal ultrasonography was normal. The fifth wave was not detected in auditory brainstem response test. Karyotype analysis was normal (46, XY). The magnetic resonance imaging (MRI) of the brain revealed absence of the lateral and third ventricles. The thalami were fused and the corpus callosum was absent. The interhemispheric fissure and falx cerebri were formed (Figs. 1, 2). There was abnormal oriented sulcus at the vertex on the left (Fig. 1). The posterior fossa and fourth ventricle were normal. The orbital MRI was also normal. All radiological features were suggestive of holoprosencephaly with no identifiable lateral or third ventricle.
Discussion
Children diagnosed with holoprosencephaly may have microcephaly, hydrocephalus, and variable degrees of mental retardation, epilepsy, endocrine abnormalities, or abnormalities of other organ systems such as cardiac, skeletal, genitourinary, and gastrointestinal. Mildly affected children may exhibit few symptoms and may live a normal life.
Holoprosencephaly can range from mild to severe and is classically classified into three types. Alobar, where the brain is not divided and there are severe abnormalities like absence of the interhemispheric fissure, single primitive ventricle, fused thalami, and absent third ventricle, olfactory bulbs and tracts and optic tracts. Semilobar, where the brain is partially divided and there are some moderate abnormalities like partially separated cerebral hemispheres and a single ventricular cavity. Lobar, where the brain is divided and there are some mild abnormalities like some fusion of structures [9].
In recent times, an unusual form of holoprosencephaly called middle interhemispheric variant has been delineated associated with a hemispheric fusion in the high frontal lobe [345].
Normally, the embryonic prosencephalon forms distinct lateral telencephalic and diencephalic structures, including the associated ventricles, olfactory and optic bulbs and tracts. The primary vesicles of the brain, the prosencephalon, mesencephalon, and rhombencephalon, are recognizable by the third embryonic week. Separate lateral telencephalic and diencephalic structures develop from a single prosencephalic vesicle, normally beginning by the fifth embryonic week of gestation [10]. Holoprosencephaly arises from a disruption of the normal induction and patterning of the rostral neural tube during early embryogenesis. Barkovich and Quint [3] described holoprosencephaly as secondary to faulty mesenchyme formation and the abnormal persistence or maldifferentiation of the primitive meningeal tissue [3].
First case of aventriculi associated with holoprosencephaly was reported by Garfinkle [6] who delineated absence of the ventricular system in an 11-year-old female with repeated aspiration pneumonitis. MRI findings were absence of the lateral, third, and fourth ventricles, and thalamic fusion, and absence of corpus callosum.
The second case was reported by Sener [8] who delineated an 1-month-old female with seizures. MRI findings were absence of supratentorial ventricles, corpus callosum and falx cerebri, fusion of the thalamus and cerebral hemispheres and hypogenetic inferior vermis and dilatation of the fourth ventricle, which is referred to as Dandy Walker variant.
The third case was reported by Kumar et al. [7] who delineated an 18-month-old male with delayed milestones. MRI findings were absence of the lateral and third ventricles, and fusion of the cerebral hemispheres posteriorly, and absence of corpus callosum.
Our case is very similar to Sener's [8] and Kumar et al.'s [7] cases but the posterior fossa and fourth ventricle were normal as in Kumar et al.'s case [7].
It is concluded that aventriculi and further anatomic variation like only thalamic fusion in our case may be seen in holoprosencephaly as a variant.

 XML Download
XML Download