

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic periodontitis is the consequence of interactions between certain subgingival microorganisms and multidimensional host reactions to infection [1]. Numerous investigations have proposed that chronic periodontitis is a potential risk factor for atherothrombotic vascular disease [2,3]. These conditions are connected because the periodontopathogens in periodontal tissues that stimulate systemic inflammation can regulate atherogenesis in periodontal disease [3]. C-reactive protein (CRP) is a serological marker of systemic inflammation that has been found to be related to increased risk for several systemic illnesses [4], and it has been proposed to be a likely mediator of the relationship between periodontitis and systemic disorders [5].
Serum amyloid A (SAA) proteins compose a group of apolipoproteins principally produced by the liver in response to cytokine release by stimulated monocytes and macrophages after an acute-phase stimulus such as infection [6]. It has been reported that elevated SAA levels may be a clinically valuable marker of cardiovascular risk, particularly in patients with periodontitis [2].
SAA and CRP are both termed first-class acute-phase reactants since they are the most sensitive plasma proteins indicating inflammatory activity [7]. Though less thoroughly investigated than CRP, SAA has also been shown to be a predictor of cardiovascular incidents [2]. Furthermore, while inflammatory markers such as CRP correlate with cardiovascular disease, the wider variety and more prompt reaction of SAA has led some researchers to propose that it may indicate a different type of acute-phase response than CRP [8,9,10]. In the current study, SAA levels were considered because of the capability of SAA to influence lipid metabolism [7] and because little information has been published about the role of SAA in periodontal disease. It is also important to note that several studies addressing SAA did not adjust for any important confounders. Dyslipidemia and blood lipids in particular have been associated with periodontitis [11]. It is therefore important to control for these variables in order to avoid biased results.
Serum levels of antibodies to various periodontal pathogens have also been linked to increased levels of inflammatory markers and the incidence of cardiovascular disease [12]. Aoki-Nonaka et al. [13] have reported that periodontal infections induced elevated levels of SAA and Porphyromonas gingivalis-specific IgG in the serum of wild-type mice. Similarly, Rivera et al. [10] have demonstrated that polymicrobial-infected mice also showed increased aortic plaque area with macrophage accumulation, SAA, and increased serum cholesterol and triglycerides, concluding that the detection of bacterial genomic DNA in the aorta and liver of infected mice and elevated levels of bacteria-specific IgG antibodies indicated a systemic infection. These findings suggest that periodontal infections or the response of the host against a periodontal infection may play a role in the pathogenesis of cardiovascular disease [12].
To the best of our knowledge, few studies have compared SAA and serum high-sensitive CRP (hs-CRP) levels as markers of systemic inflammation in periodontitis, and published studies frequently have not adjusted for confounding variables. Moreover, the present publications do not present evidence about the association of serum titers of antibodies specific to the periodontal microbiota and SAA levels in periodontitis patients. Therefore, the objectives of this investigation were to compare SAA and hs-CRP levels in patients with chronic periodontitis, and also to study the association of serum titers of antibodies specific to the periodontal microbiota and SAA/hs-CRP levels in periodontitis patients.
MATERIALS AND METHODS
Sample size calculation
The sample size was calculated to have a power of 80% and a two-tailed significance level of 0.05 for detecting a risk ratio≥1.7 for pathologic levels of SAA and hs-CRP in 94% and 54% of patients with periodontitis and in 75% and 39% of patients without periodontitis [2]. Based on these calculations, it was determined that ≥19 (for SAA) or ≥30 (for hs-CRP) persons per group would be necessary.
Patients
In this study, 61 women and 19 men with chronic periodontitis and 18 women and 12 men without periodontitis who visited the dental clinics of the Universidad de Antioquia, Medellín, Colombia, were recruited from January 2009 to December 2011. All subjects were informed individually about the objectives, risks, and benefits of the investigation and signed informed consent forms. The study design was approved by the Ethics Committee on Human Research of the School of Dentistry of the Universidad de Antioquia (ID 02-2008) according to the Declaration of Helsinki.
Systemically healthy patients with a diagnosis of chronic periodontitis were considered to be candidates for the study. All patients had at least 18 teeth, excluding third molars and teeth indicated for extraction. The diagnosis of chronic periodontitis was made according to the principles defined by Eke et al. [14]. Patients were classified as having moderate periodontitis if they had ≥2 interproximal sites with a clinical attachment level (CAL)≥4 mm, or having ≥2 interproximal sites with a probing depth (PD)≥5 mm (not at the same tooth). Severe periodontitis was defined as ≥2 interproximal sites with a CAL≥6 mm and ≥1 interproximal site with a PD≥5 mm (not at the same tooth). Individuals with no evidence of mild, moderate, or severe periodontitis were used as a control group.
The exclusion criteria, applied both to patients with periodontitis and to healthy controls, included a diagnosis of diabetes or autoimmune diseases. Pregnancy, the intake of systemic antimicrobials within the previous six months, the presence of infections or fever, a history of trauma or tooth extraction in the past six months, the use of nonsteroidal analgesics or anti-inflammatory drugs, the use of oral contraception, and previous periodontal therapy also served as exclusion criteria. Furthermore, individuals with a previous or current experience of other cardiovascular or rheumatic heart disorders or stroke were excluded. Of the 110 subjects included, 30 belonged to the control group of patients without periodontitis.
Clinical evaluation
The medical history of each patient was taken, along with clinical and radiographic examinations. The presence or absence of plaque was registered qualitatively. If bleeding occurred immediately after probing for pocket depth, the bleeding parameter was reported as positive. Both periodontitis and control subjects were asked to answer a questionnaire with regard to their socio-demographic and smoking status including gender (male or female), age (in years), smoking status (smoker or nonsmoker) and socioeconomic status (monthly personal income≥United States dollar [USD] 750; yes or no).
A trained and calibrated clinician performed all clinical examinations. Intraexaminer reproducibility was calculated before and during the study. The intraclass correlation coefficients for the mean PD and CAL were 0.92 and 0.91, respectively, and the intraevaluator kappa index was in the range of 0.85-0.96. The presence or absence of bleeding on probing and plaque was registered at all proximal, buccal and lingual surfaces, using six sites per tooth. PD and CAL were measured at all proximal, buccal and lingual surfaces to the nearest millimeter by a calibrated standard probe, using six sites per tooth (UNC-15, Hu-Friedy, Chicago, IL, USA).
Measurements of serum lipids and body mass index
Nonfasting blood samples were collected from participants at the time of the clinical examination. The diagnosis of adipose tissue disorders was made according to the criteria defined by the Third Adult Treatment Panel of the National Cholesterol Education Program [15]. To identify subjects with pathological values, the following cutoff points were used: total cholesterol≥200 mg/dL, high-density lipoprotein (HDL)<40 mg/dL in men and <50 mg/dL in women, low density lipoprotein (LDL)≥130 mg/dL, serum triglycerides>150 mg/dL, a systolic blood pressure>140 mmHg and/or a diastolic blood pressure>90 mmHg, and a body mass index (BMI≥25 kg/m2). The serum concentrations of total cholesterol, HDL cholesterol, and triglycerides were determined by fully enzymatic methods in a single local laboratory of clinical chemistry. These cutoff values are applicable to individuals with a normal risk for cardiovascular disease [15].
Anthropometric measurements such as height in meters and weight in kilograms were recorded. The BMI was calculated using the formula-BMI=weight/height2 [15].
SAA and hs-CRP concentrations
To determine SAA levels, a double sandwich enzyme-linked immunosorbent assay (ELISA) was utilized using a highly purified monoclonal antibody to human SAA (ELISA Kit KHA0012, Invitrogen Co., Camarillo, CA, USA). Obtained samples were diluted 1:200 with a standard diluent buffer and were processed according to the manufacturer's instructions. Optical densities were obtained at 450 nm in an ELISYS-1 lector and multiplied to compensate for the diluent factor. The original kit results were obtained using a standard curve and linear regression (risk ratio, 0.98), and were originally expressed in ng/mL but converted to mg/L for statistical analysis. Up to 10 mg/L of SAA was considered to be a normal value [16,17].
The samples were assessed using a LKCRP1 Kit (Immulite DPC, a division of Siemens Healthcare Diagnostics, Malvern, PA, USA). The procedure was performed according to the manufacturer's instructions (Immulite high sensitivity CRP, 2003, Siemens Healthcare Diagnostics), and the results were obtained with an Immulite 1000 analyzer (Siemens Healthcare Diagnostics). Up to 3 mg/L of hs-CRP was considered to be a normal value [16,17].
Microbial sampling
The microbial sampling of periodontitis patients was performed in pockets >5 mm deep. The deepest six pockets were designated for sampling. After removing supragingival plaque with a curette and isolating the area with cotton pellets, paper points (Maillefer, Ballaigues, Switzerland) were inserted into each periodontal pocket for 20 seconds. The paper points were transferred to a sterile tube to obtain a pool of samples for polymerase chain reaction processing and the identification of P. gingivalis, Aggregatibacter actinomycetemcomitans, and Tannerella forsythia. The polymerase chain reaction was performed as described by Ashimoto et al. [18] and Saiki et al. [19]. The reaction took place in a final volume of 25 µL, of which 5 µL corresponded to the sample and 20 µL to the reaction mixture that contained a buffer of polymerase chain reaction 1×(50-mM KCl, 10-mM Tris-HCl [pH 9.0 at 25℃], 1.5-mM MgCl2 and 0.1% Triton X-100 [Sigma-Aldrich Co., St. Louis, MO. USA]), 1.25 U of Go Taq flexi DNA polymerase (Promega, Madison, WI, USA), 1.5-mM MgCl2, 0.2 mM of each deoxyribonucleotide, and 2 µM of each primer. The temperature cycles in the thermal cycler (MyCycler Termal Cycler, Bio-Rad Laboratories Inc., Hercules, CA, USA) were performed as follows: an initial step of denaturation at 95℃ for two minutes was followed by 36 cycles at 95℃ for 30 seconds, 60℃ for a minute, 72℃ for a minute, and a final step at 72℃ for two minutes. For A. actinomycetemcomitans, the annealing temperature was changed to 55℃ and the time of the final step was increased to 10 minutes. P. gingivalis was recognized in the samples by the presence of a band corresponding to 404 base pairs (bp), T. forsythia was recognized by the presence of a band corresponding to 316 bp, and A. actinomycetemcomitans was recognized by the presence of a band at 557 bp in a 1.5% agarose gel with 0.5 µg/mL of ethidium bromide. The reference strains of each bacterium were used as positive DNA controls and the negative control was sterile water.
Indirect immunoassay (ELISA) for the determination of serum antibodies IgG1 and IgG2 to T. forsythia
Peripheral blood was collected from each subject to determine the serum levels of the IgG1 and IgG2 antibodies to T. forsythia. ELISA was performed as follows: a 96-well plate (Immulux HB, Technologies Inc., Chantilly, VA, USA) was covered with 50 µL of a 10-µg/mL concentration of sonicated P. gingivalis (TCC 33277), T. forsythia (ATCC43037) or A. actinomycetemcomitans (ATCC 29523) in a carbonate buffer (pH 9.6) and incubated overnight. The plates were blocked with 150 µL of solution of phosphate buffered saline (PBS, pH 7.2) with 1% bovine serum albumin (BSA, Sigma-Aldrich Co.), for one hour, and 1% milk and avidin (Avidin/Biotin Blocking Kit, Vector Laboratories Inc., Burlingame, CA, USA). The sera were diluted to 1/100 in PBS-Tween-BSA (1%)-biotin solution (Avidin/Biotin Blocking Kit, Vector Laboratories Inc.) and were incubated at 37℃ for an hour. Anti-IgG1 diluted to 1:5,000 (mouse antihuman IgG1, Invitrogen Co.) or anti-IgG2 diluted to 1:10,000 (mouse antihuman IgG2, Sigma-Aldrich Co.) in PBS-Tween-BSA (1%) solution, was incubated for one hour at 37℃. Streptavidin peroxidase (Invitrogen Co.) in a 1/1,500 dilution was incubated for one hour at room temperature. Between each incubation period, three washes were carried out with 250-µL PBS-tween (0.05%) solution with two minutes of stirring (Multiwasher-MW2001, SUMA, Immunoassay Center, Havana, Cuba). Finally, 50-µL phosphate/citrate buffer solution (0.5M, pH 5) was added with o-phenylenediamine (OPD Pierce, Thermo Fisher Scientific Inc., Rockford, IL, USA) and a concentration of 1 mg/mL was added and activated with H2O2 for five minutes at room temperature. The reaction was stopped with a solution of sulfuric acid (2.5M). Absorbance values were read at 490 nm (Elisa Stat Fax 2100, Awareness Technology Inc., Palm City, FL, USA). The concentration in the samples of IgG1 and IgG2 for each of the microorganisms was calculated by linear regression analysis with a known concentration curve (5-0.152 µg/mL, dilution 1:2) of human immunoglobulin IgG1 or IgG2 (Sigma-Aldrich Co.). Every sample was measured in triplicate.
Antibody titers were calculated as follows: an arbitrary serum confirmed to have a moderate antibody level judged by western immunoblotting was used as a standard, taken as one ELISA unit, and then serially diluted on every plate to generate a standard curve. As defined by Bishop et al. [20], each patient's serum was compared to the standard curve, and relative titer values were calculated correspondingly.
All microbiological and immunological laboratory procedures were performed blind, without knowledge of the clinical status of the study subjects or of the periodontal sites sampled.
Statistical analysis
The normal distribution of the continuous variables was verified with the Kolmogorov-Smirnov test. Categorical data were analyzed with the chi-square test, and the independent t-test was used to evaluate the differences between groups regarding changes in clinical parameters. In addition, the correlations of periodontal parameters with SAA/hs-CRP and between SAA and hs-CRP were determined by linear correlation analysis. Unadjusted and adjusted logistic regression analysis was carried out to determine the discriminative value of acute-phase proteins for periodontitis. Additionally, unadjusted and adjusted logistic regression analyses were carried out to determine the discriminative value of acute-phase proteins for positive antibody titers against infectious agents. Confounding variables included known individual factors: dyslipidemia (total cholesterol≥200 mg/dL, HDL<40 mg/dL in men and <50 mg/dL in women, LDL≥130 mg/dL, serum triglycerides>150 mg/dL) and BMI (<25 kg/m2 or ≥25 kg/m2) were included as dichotomous (yes or no) variables. Gender (male or female), BMI, age, smoking status (smoker or nonsmoker), hypertension (systolic blood pressure>140 mmHg and/or diastolic blood pressure>90 mmHg) and socioeconomic status (monthly personal income≥USD 750; yes or no) were also included as confounder variables. The ORs were adjusted for the above-mentioned covariates in the logistic model. The OR and corresponding 95% confidence intervals were calculated for each variable. P-values of <0.05 were considered to indicate statistical significance. All analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 depicts the periodontal parameters, socio-demographic characteristics, cardiovascular risk factors, and acute-phase reactants of patients with and without periodontitis. The socio-demographic variables did not show statistically significant differences between the two groups. Nevertheless, there was a significant difference between both groups in relation to clinical parameters (P<0.05).
Moreover, the serum levels of triglycerides were higher in periodontitis patients compared to persons without periodontitis (178 mg/dL vs. 165 mg/dL, P<0.05) and the HDL levels were lower (44 mg/dL vs. 50 mg/dL, P<0.05) (Table 1). Moreover, in periodontitis patients, SAA concentrations were higher than in the controls (P=0.03), and serum hs-CRP levels were also higher in periodontitis patients than in the controls, with a greater degree of statistical significance (P=0.009) (Table 1).
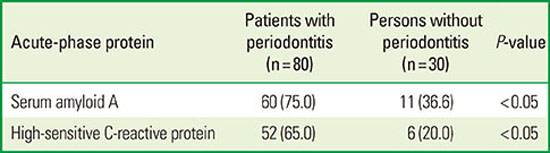
Table 2 shows the number and the percentage of periodontitis patients and individuals without periodontitis with elevated SAA and hs-CRP levels. Higher levels of SAA and hs-CRP were observed in periodontitis patients (P<0.05).
The Spearman correlation analysis between acute-phase proteins showed that SAA positively correlated with hs-CRP (r=0.218, P=0.02). Moreover, the Spearman correlation analysis between acute-phase proteins and periodontal parameters showed that SAA was positively correlated with PD and the presence of plaque. Instead, hs-CRP was positively correlated with CAL (Table 3).
The occurrence of the periodontal pathogens we investigated is listed in Table 4. The prevalence of T. forsythia and P. gingivalis was higher in the group of patients with periodontitis. Neither hs-CRP nor SAA was associated with the presence of any microorganism.
Increased serum levels of IgG2 antibody to P. gingivalis were also observed to be associated with chronic periodontitis (P=0.006). However, no associations were found between chronic periodontitis and serum levels of IgG1 antibody to P. gingivalis, IgG antibody to T. forsythia, and IgG antibody to A. actinomycetemcomitans.
In bivariate analysis, high levels of hs-CRP (>3 mg/L) and SAA (>10 mg/L) were significantly associated with chronic periodontitis (P=0.004). With these data, we analyzed the association between periodontitis and both acute-phase proteins using a logistic regression model adjusted for age, gender, socioeconomic status, smoking, BMI, blood pressure, HDL, LDL, total cholesterol, and triglycerides.
In the unadjusted model, chronic periodontitis was associated with high levels of SAA. This statistically significant association remained after adjustment for possible confounders (Table 5). Similarly, in the unadjusted model, chronic periodontitis was associated with high levels of hs-CRP. This statistically significant association also remained after adjustment for possible confounders (Table 5).
Interestingly, in bivariate analysis, high SAA and hs-CRP were significantly associated with increased serum levels of IgG2 antibody to P. gingivalis (P=0.004 and P<0.001, respectively). With this information, we investigated the association between periodontitis and both acute-phase proteins using a logistic regression model adjusted for age, gender, socioeconomic status, smoking, BMI, blood pressure, HDL, LDL, total cholesterol, and triglycerides.
The unadjusted OR for the association between increased serum levels of IgG2 antibody to P. gingivalis and high SAA was 5.14 (P=0.003). This association, although somewhat attenuated, remained significant after adjustment for possible confounders (Table 6). Similarly, in the unadjusted model, increased serum levels of IgG2 antibody to P. gingivalis were associated with high hs-CRP. This statistically significant association also remained after adjustment for possible confounders (Table 6).
DISCUSSION
To the authors' knowledge, this is the first study to compare SAA and hs-CRP as markers of systemic inflammation in periodontitis, controlling for several confounders. Cardiovascular disease and an increased acute-phase reaction with elevated levels of CRP and SAA share various common risk factors involving smoking, high BMI, and older age [4,7]. The progression of cardiovascular disease and periodontitis seems to overlap with respect to some essential risk factors, including increased systemic levels of proinflammatory acute-phase reactants such as SAA and CRP [2,4].
It has been proposed that extended exposure and augmented levels of systemic inflammatory mediators may be the cause of increased cardiovascular risk in patients with periodontitis [21]. Proinflammatory cytokines stimulate hepatocytes to generate acute-phase proteins [22], which are elevated in otherwise healthy adults with mild periodontal conditions [23].
The present research showed that chronic periodontitis was discriminatively related with elevated levels of SAA and hs-CRP. Similar results have previously been reported for CRP in periodontitis [23] and for SAA [24] in coronary heart disease. As pointed out by Pearson et al. [17], periodontal infection can result in underdiagnosed chronic inflammation, which contributes to systemic inflammatory responses and may raise the risk for cardiovascular disease.
In this investigation, SAA levels were significantly higher in patients with chronic periodontitis than in individuals without periodontitis. Similarly, hs-CRP levels were significantly elevated in periodontal patients compared to healthy patients. Glurich et al. [2] assessed the SAA and CRP levels of four groups of patients: those with only periodontal disease, only cardiovascular disease, both diseases, and neither condition. Their results were controversial: higher levels of SAA (15.9 mg/L) were observed in healthy individuals than in periodontal patients (11.15 mg/L). However, CRP levels<3 mg/L were found in both healthy subjects and periodontitis patients. Various factors might explain their results. First, a classification bias may be present because they selected periodontal patients who showed a mean attachment loss≥4 mm, without considering PD; similarly, patients were considered to be healthy if they presented a mean attachment loss≤2 mm, without considering PD. Second, they did not adjust for various potential confounders, except for smoking.
Earlier polymicrobial periodontal disease models in mice showed that periodontal infection produced elevated SAA levels [10,13]; however, limitations are undeniably present when applying conclusions from mice models to human periodontitis patients.
Graziani et al. [25] and Vuletic et al. [26], assessed serum markers of systemic inflammation in periodontitis patients before and after nonsurgical therapy, and before and after full mouth tooth extraction, respectively. However, neither study used a healthy control group, which makes it difficult to compare their results with our research. Graziani et al. [25] demonstrated that serum levels of CRP and SAA were elevated within 24 hours of treatment, but normalized after 30 days. Likewise, Vuletic et al. [26] showed that SAA levels were reduced three months after treatment. SAA levels have been shown to positively correlate with the progress of atherosclerosis [27], implying that a prolonged elevation of SAA concentrations resulting from periodontitis may directly or indirectly contribute to the progress of cardiovascular disease. SAA, which is physically present on HDL, may play an important role in binding lipoproteins to the vessel wall, thus contributing to lipoprotein oxidation and the progress of atherosclerotic lesions [28]. Consequently, higher levels of SAA in a subgroup of patients may indicate an elevated risk for cardiovascular disease, compared to periodontitis patients with normal SAA concentrations [26].
The studies presented above show that SAA has only begun to be studied in dentistry. Additionally, the experimental designs of the above studies do not permit a proper comparison with the present study. Moreover, appropriate comparisons between SAA and CRP have not yet been made in periodontal research. However, although it is less studied than CRP, SAA has also been shown to be a predictor of cardiovascular events, and both acute-phase reactants have been widely compared in medicine more broadly [9,24,29,30].
Contrastingly, studies of CRP in periodontitis are abundant. Statistically significant increases in CRP levels have been observed in patients with periodontitis compared to healthy controls [4,5,30,31,32,33], as was found in the present investigation. Our results were corroborated by Slade et al. [32], who reported CRP levels of 4.5 mg/L in periodontitis patients. Similarly, Noack et al. [30] presented mean values for CRP of 4.06 mg/L and 1.70 mg/L in periodontitis patients and healthy individuals, respectively.
In the current study, approximately 36% of patients without periodontitis and 75% of periodontitis patients had SAA concentrations higher than 10 mg/L, which are considered abnormally high values [16,17]. Glurich et al. [2] reported corresponding percentages of 54% and 63% in healthy individuals and in periodontitis patients, respectively. These results suggest that SAA may be able to detect a higher number of patients with cardiovascular risk compared to hs-CRP. The postinfarction monitoring of SAA levels has shown that SAA is the best marker for predicting the incidence of complications and death in patients with cardiovascular disease [34]. Thus, elevated SAA concentrations may be a clinically valuable indicator of cardiovascular risk, particularly in patients with periodontitis [2].
The present study demonstrated a significant positive correlation between SAA and hs-CRP. Furthermore, a significant correlation has also been observed in cardiovascular studies [33,34]. Both CRP and SAA are regularly used clinically as inflammatory markers in cardiovascular disease. These proteins frequently react in parallel to a particular stimulus; however, the magnitude of the SAA response has been shown to be greater than that of CRP [34].
A significant positive correlation of SAA and hs-CRP with PD and CAL, respectively, was also observed in this study. Such correlations have also been detected for CRP in periodontal research [5,30]. However, Vuletic et al. [26] showed that SAA levels did not show a statistically significant correlation with any pretreatment periodontal disease parameters. Further studies are necessary to firmly establish the correlation between SAA and periodontal parameters.
The clinical characteristics of periodontitis result from a microorganism infection and the host response. Direct measures of the infection, comprising the quantification of subgingival bacteria and antibody responses to these periodontopathogens, have been recommended as a more correct metric of periodontitis for investigations of the relationship between periodontal and systemic disease [35]. Correspondingly, the main results of the present investigation were that periodontitis and IgG2 antibody to P. gingivalis were independently associated with higher concentrations of SAA and hs-CRP, controlling for various potential confounders (Tables 5, 6). Pitiphat et al. [5] obtained similar results concerning the association between periodontitis and CRP, and Dye et al. [12] presented comparable conclusions regarding the association between CRP and antibodies to P. gingivalis. Corresponding to our results, Craig et al. [36] also documented an association between CRP and IgG to P. gingivalis, but not to titers of antibodies to five other periodontal pathogens, including A. actinomycetemcomitans.
As was suggested previously, the association between antibody response to P. gingivalis and high CRP levels supports the hypothesis that periodontal infections can contribute to systemic inflammation and thereby to atherosclerosis and cardiovascular disease [12]. As well, the serological study of the periodontal microbiota allows possible markers of periodontal infection to be monitored, and the concentrations of these antibody responses may help to distinguish between states of simple bacterial colonization and infection [12].
The extant literature contains sparse information about the association of serum titers of antibodies to periodontal microbiota and SAA levels in periodontitis patients. Aoki-Nonaka et al. [13] have shown that experimental periodontal infection induces elevated serum levels of SAA and P. gingivalis-specific IgG. Moreover, Rivera et al. [10] have demonstrated that polymicrobial-infected mice also present an increased aortic plaque area with macrophage accumulation, elevated SAA, and increased serum cholesterol and triglycerides. The presence of P. gingivalis elevated serum levels of IgG antibody in polymicrobial-infected mice approximately 100,000 folds compared to the levels in the control mice. They concluded that increased levels of SAA are an indicator of the role of periodontopathogens in cardiovascular disease.
The present study has several strengths. First, the control group was comparable with the periodontal patients regarding all socio-demographic characteristics. Second, the study controlled for a large number of confounding variables. However, one limitation was that the results were obtained from a cross-sectional study design to explore and compare factors correlated with augmented levels of SAA and hs-CRP, which prevents a classic exploration of causality. Nonetheless, SAA and hs-CRP were found to be associated with periodontitis and IgG antibody to P. gingivalis, after adjusting for various potential confounders.
In conclusion, our results suggest that SAA and hs-CRP concentrations are comparably elevated in patients with chronic periodontitis. Our results demonstrated that a high serum titer of IgG antibody to P. gingivalis and the presence of periodontal disease is independently related to high SAA and CRP levels. This is the first investigation to establish that SAA and hs-CRP have similar levels in patients with chronic periodontitis, suggesting that both are good markers of inflammation in such patients. Future studies designed to provide epidemiological confirmation of these findings are recommended.





 XML Download
XML Download