

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
One of the necessary requirements for a dental implant is the presence of at least a moderate amount of bone in order to place an implant with the appropriate length and diameter. The loss of the alveolar ridge due to trauma, periodontal disease, or the failure of endodontic treatment, however, may make it difficult to place the implant in the best location for proper esthetics and function. The maxillary posterior area, is known to be especially difficult for implant treatment and to have a low success rate because of the poor bone quality. Moreover, the posterior edentulous maxilla has represented a challenge for clinicians owing to the resorption of the alveolar ridge and pneumatization of the maxillary sinus.
This has led to the development of a bone augmentation technique, the onlay bone graft and sinus augmentation. Sinus augmentation via lateral window osteotomy has been routinely performed in the last few years and has been regarded as a predictable procedure [1-4]. However, the choice of the bone graft material is still under discussion.
The use of autogenous bone in sinus augmentation has been regarded as a superior method because of the reproducible healing mechanism of osteogenesis, osteoinduction, and osteoconduction. Nevertheless, there are some limitations, e.g., the need for additional surgical sites and the rapid resorption rate when the autogenous bone is used as a sinus grafting material [5-7]. Therefore, the use of synthetic bone has been recently appraised for its biocompatibility and volume maintenance capacity [8,9].
Various synthetic materials have been developed for use in maxillary sinus augmentation to allow bone ingrowth and to prevent sinus pneumatization after grafting. Among them, the mixture of hydroxiapitite (HA) and beta-tricalcium phosphate (β-TCP) has been studied extensively as a new alloplastic material [10]. HA can play an osteoconductive role due to its appropriate space maintenance capacity, but it has a low-grade osteogenetic property. On the other hand, β-TCP, with its good biocompatibility, has been used as a substitute for autogenous bone [11,12]. In light of this, mixing adequate ratios of HA and β-TCP allows for controlling the resorption rate without distorting its the bone's osteoconductive property [13-15].
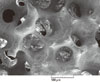
Osteon (Dentium, Seoul, Korea) is synthetic material containing 70% HA and 30% β-TCP. It has a porous structure, which can accelerate new bone ingrowth and maturation (Fig. 1). Two different particle sizes of Osteon have been used (0.5-1.0 mm and 1.0-2.0 mm). In several previous studies, Osteon was regarded as a suitable sinus augmentation material based on histologic analysis [16]. Moreover, we have previously reported on the volume maintenance of grafted Osteon and implant success rate in a pilot study [17]. In that study, the grafted material was well maintained in the sinus and decreased slightly over 1 year (0.05 mm/month). It is suggested that Osteon may produce predictable results when it is used as a grafting material for sinus floor augmentation.
The aim of the present study was to evaluate the cumulative survival rate (CSR) of implants placed in sinuses augmented with Osteon, and to assess the resorption rate of the grafted material radiographically with increased sample size and statistical power as an extension to our previous studies.
CASE DESCRIPTION
This study was approved by the Institutional Review Board of Yonsei University College of Dentistry (Approval No. 5-2008-3). A total 45 implants were placed in 20 maxillary sinuses of 20 patients (8 males, 12 females, mean age 57.2±11.3 years) with the condition of having under 5 mm of residual alveolar bone height, using a sinus augmentation technique via lateral window osteotomy [18]. All implants were maintained with at least 6 months of prosthetic loading time. Patients' exclusion criteria were: 1) heavy smoking (more than 20 cigarettes per day), 2) a debilitating systemic disease such as uncontrolled diabetes mellitus 3) signs and symptoms of maxillary sinus disease, or 4) active periodontal disease involving the residual dentition.
Five implants were from Branemark System-MKIII TiUnite (NobelBiocare AB, Gotenborg, Sweden); 12 implants were from Xive (Dentsply Friadent, Mannheim, Germany), 5 implants were from Astra (Astra Tech AB, Mölndal, Sweden), 6 implants were from Osstem GSII (Osstem Implant Co., Busan, Korea), and 17 implants were from Implantium (Dentium). Five implants had a machined surface; 29 implants had a sandblasted, large-grid and acid etched surface; and 11 implants had a resorbable blast media surface. All implants were placed in either one- or two-stage surgery. The timing of implantation was determined, depending on the primary stabilization of implants. In the two-stage approach, implantation was performed 6 months after the augmentation of the maxillary sinus.
A mixture of 2 different types of Osteon in a 1:1 ratio was used in 10 patients, while only the larger particle size of Osteon was used in the other 10 patients. The quality of bone was evaluated according to Lekholm and Zarb's classification during the surgical procedure [19]. Most of the examined subsinus ridges were composed of bone with poor quality (type III and IV). General information on each case is presented in Table 1.
Surgical technique
A modified Caldwell-Luc sinus augmentation was performed under local anesthesia (2% lidocaine hydrochloride-epinephrine 1:100,000; Huons Co., Seoul, Korea) [20,21]. In brief, the surgical area was prepared via elevation of a full thickness muco-periosteal flap. Osteotomy was performed at the lateral surface of the sinus wall using a diamond round bur and piezoelectric device (Piezosurgery, Mectron Spa, Carasco Genova, Italy) and the sinus membrane was carefully lifted. The sinus cavity was then packed with Osteon, and the lateral window was covered by an absorbable sponge (Collatape, Zimmer Dental, Calsbad, CA, USA). The muco-periosteal flap was repositioned and sutured with absorbable suture material (Monosyn 4.0 Glyconate Monofilament, B. Braun Melsungen AG, Melsungen, Germany; Vicryl 5.0 Polylactim, Johnson & Johnson, New Brunswick, NJ, USA). The prosthodontic procedure was completed after a mean healing period of 6-12 months.
Radiographic analysis
The radiographic analysis was performed by panoramic radiographs and intraoral radiographs using software (Starpacs, Infinitt Co., Seoul, Korea). All the values were calibrated precisely based on the length of the implant fixture, and these were double checked by a single investigator. At least 2 consecutive panoramic radiographs were taken--one immediately after the sinus augmentation, the other 1 year after the surgery. Additional radiographs were obtained every 6 to 12 months through the follow-up period. The linear measurements taken from radiographs were described below (Fig. 2).
The original alveolar bone heights prior to the surgery [24], from the alveolar crest to the base of the sinus were measured (Table 1). The augmented sinus heights (ASH) were measured from the 1st bone to implant contact points to the base of the maxillary sinus, which was elevated with Osteon at the mesial and distal aspects of the implants. The volume of marginal bone loss (MBL) was obtained compared with the intraoral radiographs immediately taken after the surgery and 1 year postoperatively. The reduced height of Osteon (RHO) was calculated based on the changes in the ASH and MBL.
Statistical analysis
The individual mean values were calculated. Differences in RHO according to the timing of implantation and the type of Osteon were analyzed using a independent t-test. A one way analysis of variance was used to evaluate the difference in RHO according to the implant sites. A post-hoc Scheffe test was used to evaluate the differences between groups. A P value of <0.05 was considered significant. Correlation between the RHO and follow-up period were determined by Spearman's test. SPSS ver. 12.0.0 (SPSS Inc., Chicago, IL, USA) was used for all of the statistical analyses.
Implant survival rate
No complications, including wound dehiscence and sinus membrane perforation, were observed in any of the patients. Two of the 45 implants were removed between implantation and the follow up period (case 2, I16, 17). All loss of implants occurred prior to prosthetic loading. Both cases were successfully restored by wider diameter implants. The 0 to 6 month CSR was 95.56%, and this value continues to 42 months (Table 2).
Radiographic results
The mean follow up period for implants after the sinus augmentation was 19.4 months (range, 12 to 42 months). The original sinus height was a mean of 4.3 mm (range, 2.5 to 5.8 mm) and the augmented sinus height was a mean of 13.4 mm (range, 9.81 to 18.1 mm) after the surgery. The mean crown/Implant ratio was 1.19±0.24 mm which was relatively higher than the natural molar. The marginal bone loss up to 12 months was measured as 0.29±0.42 mm and up to 42 months as 0.52±0.56 mm. The RHO 1 year postoperatively was 0.83±0.38 mm, and at 42 months postoperatively was 0.88±0.39 mm (Table 3). No significant correlation was noted between the RHO and follow up periods by Spearman's test (P=0.102). There were no statistically significant differences in the reduced height of Osteon depnding on simultaneous or delayed implantation (P=0.299; Table 4) and particle size of the Osteon (P=0.644; Table 5). In addition, no significant difference in the RHO was observed according to the site of implantation (P=0.527; Table 6).
DISCUSSION
An ideal material for maxillary sinus augmentation should provide biocompatibility to allow bone ingrowth and have a space maintaining property to prevent sinus pneumatization [24]. In the results of the present study, the grafted Osteon was well maintained in the sinus and decreased slightly over a 3.5-year time period, demonstrating that it is a clinically suitable material for sinus augmentation.
Some volumetric loss of grafted material is unavoidable because of the air pressure from respiration in the maxillary sinus regardless of the type of material used [2,25,26]. Therefore, the change in the height of the grafted material is an important factor for implant stability.
Previous studies about the loss of grafted material have been mixed. Hatano et al. [27] used autogenous bone and xenogenous bone mixed at a ratio of 2:1 for sinus augmentation with simultaneous implant placement and evaluated the resorption rate. They reported that statistically significant resorption had occurred after 2-3 years, and the maxillary sinus floor was observed at a similar level or slightly below that of the implant apex. On the other hand, Maiorana et al. [28] evaluated the resorption rate after 4 years of maxillary sinus augmentation using synthetic bone graft material (hydroxyapatite and collagen). The survival of implants was 97% and the grafted material remained steady, showing a 0.5-1 mm resorption height. Generally, it was reported that the resorption rate is influenced by the type of graft material [2]. The resorption rate was 1.76 mm in autograft, 2.09 mm in allograft (freeze-dried demineralized bone), and 0.96 mm in alloplast (hydroxyapitite).
The maxillary sinus cavity is a kind of contained defect surrounded by sinus basal bone and the Schneiderian membrane; thus it has excellent healing potential even without bone graft materials. From this perspective, the long-lasting synthetic and xenogenic bone materials are considered to be a better choice in terms of material resorption.
Two out of 45 implants were removed in this study before prosthetic loading, so this can be regarded as an early failure. It seems that excessive hematoma causes the formation of exuberant granulation tissue, which can be detrimental to initial osseointegration. The overall CSR was 95.56%, and this result was comparable with other studies despite the small sample size [1-4].
The reduction in volume of the Osteon was higher than in our previous report (0.48 mm resorption in 13 months) [17]. No significant difference in the reduced volume of the Osteon was observed according to the timing of implantation. From our previous studies, it was reported that the largest amount of Osteon resorption occurred in the 1st molar area and the augmented sinus membrane was changed from a convex shape to a flat shape. In this study, however, there was no correlation between the area of the implantation and the resorption rate.
Interestingly, the resorption of Osteon occurred regardless of the flow of time. In most other papers, it was found that the graft materials might undergo gradual resorption and pneumatization by time [2,27]. Hieu et al. [29] radiographically evaluated the changes in height of the xenogenic materials (Bio-Oss, Geistlich Sons, Wolhusen, Switzerland; OCS-B, Nibec, Seoul, Korea) after maxillary sinus augmentation over the course of 2 years. This study reported that significant material resorption can take place over time. Nonetheless, it could be assumed that many other factors, e.g., the air pressure in the maxillary sinus, the form of augmented material, and the density of the grafted material, are more important than the time flow. Therefore, it is possible that the resorption rate of the grafted material is affected by the host's environment. This would be expected to be clarified with further study.
Two dimensional panoramic radiographs have been used to evaluate the grafted material and its relationship with implants
[27,30,31]. Recently, a study utilizing computed-tomography and magnetic resonance imaging assessed the grafted sinus floor and this showed more accurate results on the volumetric change [32]. However, in the present study, we used only 2-dimensional images; thus further study using 3-dimensional images would provide a more accurate volumetric measurement of Osteon.
Within the limitations of this study, it can be suggested that Osteon may have predictable results when it was used as a grafting material for sinus floor augmentation due to its excellent osteoconductive property.







 XML Download
XML Download