

 PDF
PDF ePub
ePub Citation
Citation Print
Print


STATE OF THE ART IN THE TREATMENT OF VENOUS THROMBOEMBOLISM
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are important pathologies that affect apparently healthy individuals as well as medical or surgical patients. Therapeutic objectives are essentially the prevention of thrombus extension and embolization, and the prevention of recurrent episodes of venous thromboembolism (VTE) to reduce the risk of fatal pulmonary emboli. Despite the availability of different treatment strategies, the large majority of patients commonly receive a similar therapeutic approach, and the choice of the treatment is eventually influenced by the severity of the presentation of the disease. Anticoagulation is the main therapy for acute VTE and the evidence for the need for anticoagulation in these patients is based on the results of clinical studies performed more than 40 years ago [1]. Patients need to start treatment as soon as the diagnosis is confirmed by objective testing, and because anticoagulant drugs with a rapid onset of action are needed in this phase, three parenteral therapeutic options are currently available for initial treatment: unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and fondaparinux [2]. Fondaparinux is a synthetic pentasaccharide that inhibits factor Xa indirectly by binding to antithrombin with high affinity and was recommended for the first time in the 8th edition of the American College of Chest Physicians (ACCP) Guidelines on Antithrombotic and Thrombolytic Therapy, which is the most recent and was published in 2008 [2]. This recommendation was based on the results of the MATISSE studies [3, 4]. In the MATISSE DVT study [3], 2205 patients with DVT were treated with a once daily subcutaneous dose of fondaparinux (7.5 mg for patients weighting 50 to 100 kg, 5.0 mg for patients weighting less than 50 kg and 10.0 mg for patients weighting more than 100 kg) or with a twice daily subcutaneous dose of enoxaparin (1 mg/kg) for at least five days. There were no differences in the incidence of recurrent VTE at 3 months (3.9% vs 4.1%), major bleeding while on treatment (1.1% vs 1.2%), and mortality at 3 months (3.8% vs 3.0%). In the MATISSE PE study [4], 2213 patients with acute PE were randomly allocated to treatment with subcutaneous fondaparinux or intravenous UHF. Recurrence of VTE at 3 months (3.8% vs 5.0%) and major bleeding while on treatment (1.3% vs 1.1%) were again similar between the two groups.
In selected cases, more aggressive treatment strategies are required. There is widespread agreement that patients with PE resulting in cardiogenic shock initially treated with thrombolysis plus anticoagulation have better short- and long-term clinical outcomes than those who receive anticoagulation alone [5]. More recently, some authors have proposed that thrombolysis should be administered to patients with normal blood pressure (and no contraindications) when clinical or echocardiographic evidence of right ventricular dysfunction is present. In the most recent ACCP guidelines [2], the use of thrombolytic therapy, which was previously recommended for hemodynamically unstable patients (massive PE) only, is now also suggested for selected high-risk patients without hemodynamic instability and with a low risk of bleeding, with a grade 2B recommendation. However, this remains a controversial issue, and the controversy is likely to remain at least until the results of an ongoing European trial, in which 1,000 PE patients with preserved systolic blood pressure, elevated troponin levels, and right ventricular enlargement on echocardiography are randomised to thrombolytic therapy (tenecteplase plus heparin) versus heparin alone, will become available. Other guidelines, such as those of the European Society of Cardiology, currently do not recommend routine use of thrombolysis in non-high-risk patients [6].
As soon as possible after the diagnosis of VTE, most patients are also started on oral anticoagulant treatment with vitamin K antagonists for the long-term secondary prevention of the disease. Because of their slow onset of action, and because of their potential to paradoxically increase the prothrombotic state of the patient by also inhibiting endogenous anticoagulants such as protein C, vitamin K antagonists can not be used as the only treatment strategy during the acute phase of disease and thus require initial association with parenteral anticoagulants for a minimum of 5 days. After this period, oral anticoagulant therapy alone is continued until its benefits (reduction of recurrent VTE) no longer clearly outweigh its risks (increase in bleeding). The risk of recurrence after stopping therapy is largely determined by two factors: whether the acute episode of VTE has been effectively treated; and the patient intrinsic risk of having a new episode of VTE. Therefore, guidelines suggest to treat VTE for at least 3 months if transient risk factors are identified and to consider long-term treatment for patients with unprovoked proximal VTE and no risk factors for bleeding, in whom good quality anticoagulant monitoring is achievable [2]. When the risk to benefit ratio remains uncertain, patient preference to continue or to stop treatment should also be taken into account. VTE is defined unprovoked if cancer or a reversible provoking risk factor is not present. Reversible provoking factors include major risk factors such as surgery, hospitalization, or plaster cast immobilization, if within 1 month; and minor risk factors such as surgery, hospitalization, or plaster cast immobilization, if they have occurred 1 to 3 months before the diagnosis of VTE, and estrogen therapy, pregnancy, or prolonged travel (i.e. more than 8 hours). The greater is the impact of the provoking reversible risk factor (e.g., recent major surgery) on the risk of VTE, the lower is the expected risk of recurrence after stopping anticoagulant therapy. Of interest, in the most recent version of the ACCP guidelines, the presence of thrombophilia is no longer considered for the risk stratification of the patients.
For the secondary prevention of VTE in patients with active cancer, the use of LMWH for the first 3 to 6 months is now preferred over the use of vitamin K antagonists [2]. This recommendation is based on the results of three studies that selectively enrolled a total of 1,029 patients with VTE in association with active cancer and that found that, compared to oral anticoagulant therapy with vitamin K antagonists, 3 months or 6 months of therapeutic-dose LMWH was associated with less recurrent VTE in one study and less bleeding in another study (relative risk for the three studies: recurrent VTE, 0.56; 95% CI, 0.38-0.82; major bleeding, 1.01; 95% CI, 0.62-1.64; mortality, 0.92; 95% CI, 0.78-1.10) [7-9]. LMWH is usually administered at full therapeutic dose for the first month and then reduced at approximately 75% of the initial dose thereafter.
NEW STRAEGIES TO INDIVIDUALIZE THE DURATION OF SECONDARY PREVENTION
There is a trend toward a more extended duration (potentially life-long) of secondary prevention for a large proportion of patients with a first episode of VTE, namely those with an unprovoked proximal DVT or PE who have a low risk of bleeding and those with a permanent risk factor such as cancer [2]. Indeed, given the high rate of VTE events still defined as unprovoked, which ranges between 26% and 47% [10], this recommendation has an enormous potential impact on the long-term management of patients with VTE and on related costs. To overcome this problem, there is an increasing interest in the use of clinical prognostic factors to assist clinicians in individualizing the optimal duration of secondary prevention of unprovoked VTE. These include the measurements of D-dimer and of residual venous obstruction at ultrasound. These strategies, although still not widely accepted, are now supported by the results of randomized clinical trials and of large cohort studies [11-16]. In the PROLONG study [11], patients with unprovoked VTE underwent D-dimer testing 1 month after oral anticoagulant treatment discontinuation. Patients with a normal D-dimer level did not resume anticoagulation, whereas those with an abnormal D-dimer level were randomly assigned either to resume or to discontinue treatment. The D-dimer assay was abnormal in 36.7% of patients. The rate of recurrences was 15.0% among the 120 patients who stopped anticoagulation as compared with 2.9% among the 103 patients who resumed anticoagulation, for an adjusted hazard ratio of 4.26 (95% confidence interval, 1.23-14.6). VTE recurred in 6.2% of patients with a normal D-dimer level. Because D-dimer levels may increase over time and a single normal D-dimer may be inadequate to predict a low risk of recurrence, the same group carried out a second study, the PROLONG II study, with the aim to assess the time course of D-dimer and its relation with late recurrences in patients with normal D-dimer 1 month after anticoagulation suspension for a first episode of unprovoked VTE [12]. This study showed that when D-dimer becomes abnormal at the third month and remains abnormal afterward, the risk of recurrence is higher than in patients in whom D-dimer remains normal at the third month and afterward (adjusted hazard ratio: 7.9; 95% confidence interval: 2.1-30).
Two randomized controlled studies have evaluated the role of residual vein thrombosis to predict the risk of recurrent VTE [15, 16]. In the first study, patients with a first episode of DVT were managed according to ultrasound findings after an initial course of oral anticoagulant treatment. Patients with evidence of residual vein thrombosis were randomized to either stop or continue anticoagulants for 9 additional months, whereas patients without residual vein thrombosis treatment was stopped [15]. Residual thrombosis was detected in 69.8% of patients; recurrent events occurred in 27.2% of those who discontinued (15.2% person-years) and 19.3% of those who continued oral anticoagulant treatment (10.1% person-years). The relative adjusted hazard ratio was 1.58 (95% confidence interval 0.85-2.93). Of the 30.2% patients without residual thrombosis, only 1.3% (0.63% person-years) had a recurrence. In the second study, 538 patients with a first episode of acute proximal DVT at completion of an uneventful 3-month period of anticoagulation were randomly assigned to fixed-duration anticoagulation (no further anticoagulation for secondary thrombosis and an extra 3 months for unprovoked thrombosis) or flexible-duration, ultrasonography-guided anticoagulation (no further anticoagulation in patients with recanalized veins and continued anticoagulation in all other patients for up to 9 months for secondary DVT and up to 21 months for unprovoked thrombosis) [16]. Overall, 17.2% of the patients allocated to fixed-duration anticoagulation and 11.9% of the patients allocated to flexible-duration anticoagulation developed recurrent VTE (adjusted hazard ratio, 0.64; 95% confidence interval 0.39-0.99). For patients with unprovoked DVT, the adjusted hazard ratio was 0.61 (95% confidence interval 0.36-1.02) and 0.81 (95% confidence interval 0.32-2.06) for those with secondary DVT.
NEW ANTICOAGULANTS FOR THE TREATMENT OF VENOUS THROMBOEMBOLISM
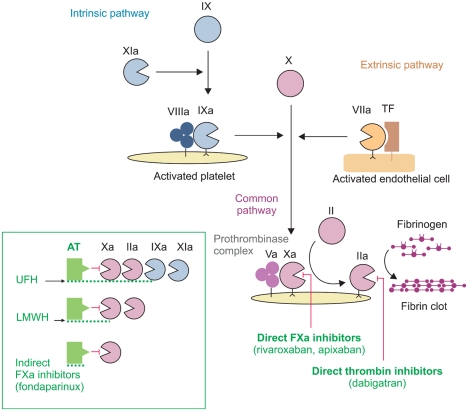
The approach to the development of new anticoagulants as alternatives to heparins and vitamin K antagonists has been guided by the requirement for convenient administration with predictable pharmacokinetics, pharmacodynamics and a wide therapeutic window that would permit fixed dosing without requiring coagulation monitoring. Research has in particular focussed on targeting thrombin (Factor IIa) and Factor Xa, which are common to both the intrinsic and extrinsic coagulation pathways (Fig. 1). Thrombin inhibitors act to prevent fibrin formation, as well as inhibiting thrombin-mediated activation of Factors V, VIII, XI and XIII, and platelets. Inhibitors of Factor Xa act at an earlier stage in the cascade, they can inhibit both free and prothrombinase-bound Factor Xa and are also able to inhibit clot-associated Factor Xa, thus preventing clot-associated Factor Xa from activating prothrombin and thereby contributing to the procoagulant activity of thrombi and therefore to the propagation of the thrombus [17].
1. Direct thrombin inhibitors
Dabigatran etexilate is an univalent direct thrombin inhibitor that binds exclusively to the active site of thrombin with the advantage, in comparison with heparins, to inactivate fibrin-bound thrombin. Moreover, dabigatran etexilate is a reversible direct thrombin inhibitor, which dissociates relatively quickly from thrombin, leaving a small amount of free, enzymatically active thrombin available for control of haemostasis. Dabigatran etexilate, is the prodrug of dabigatran, is rapidly absorbed from the gastro-intestinal tract and has a rapid onset of the anticoagulant activity, with plasma levels peak at 2 hours [18]. The half-life ranges between 12 and 17 hours [18]. Dabigatran produces a predictable anticoagulant effect, requires no coagulation monitoring and can be given once daily. It prolongs the activated partial thromboplastin time, but its effect is not dose-linear and it is not suitable for a precise quantification of the anticoagulant effect. At least 80% of dabigatran is excreted unchanged via the kidneys; therefore, the drug is contraindicated in patients with severe renal failure, with a creatinine clearance less than 30 mL/min [18]. Dabigatran etexilate has been already licensed in the European Union and in Canada for the prevention of VTE in patients undergoing hip- and knee-replacement surgery, with a recommended dose of 220 mg once daily for all patients but those with moderate renal insufficiency (creatinine clearence between 30 and 50 mL/min) and the elderly (aged 75 or more), for whom the recommended dose is 150 mg once daily [19]. A dose reduction is also recommended for patients on amiodarone treatment [19].
Dabigatran etexilate is currently undergoing a large phase III program for the evaluation of its efficacy and safety in the acute treatment end in the secondary prevention of VTE. The RE-COVER trial evaluated dabigatran for 6 month treatment of acute symptomatic VTE, while the RE-MEDY and the RE-SONATE trials are recruiting patients who have been successfully treated with standard doses of an approved anticoagulant for three to six months or who have completed 6 to 18 months of treatment with vitamin K antagonist for confirmed acute symptomatic VTE, respectively. The RECOVER study was published at the end of 2009 [20]. Patients with acute VTE, DVT and/or PE, who were initially treated with parenteral anticoagulants, were randomized to receive dabigatran etexilate, administered at a dose of 150 mg twice daily, or dose adjusted warfarin (international normalized ratio of 2.0 to 3.0). The primary outcome of the study was the 6-month incidence of recurrent symptomatic, objectively confirmed VTE and related deaths. Thirty of the 1,274 (2.4%) dabigatran patients, as compared with 27 of the 1,265 (2.1%) warfarin patients, had recurrent VTE. The difference in risk was 0.4 percentage points (95% confidence interval, -0.8-1.5). The hazard ratio with dabigatran was 1.10 (95% confidence interval, 0.65-1.84). Major bleeding episodes occurred in 20 (1.6%) dabigatran patients and in 24 (1.9%) warfarin patients (hazard ratio with dabigatran, 0.82; 95% CI, 0.45-1.48), and episodes of any bleeding were observed in 205 (16.1%) dabigatran patients and in 277 (21.9%) warfarin patients (hazard ratio with dabigatran, 0.71; 95% confidence interval, 0.59-0.85).
2. Direct factor Xa inhibitors
Rivaroxaban is the first of this new class of drugs. It is a potent and selective oral Factor Xa inhibitor with a particular chemical structure in its active-site binding region that plays a role in the oral absorption of the drug, with a relatively high bioavailabity (nearly 80%) [21]. Plasma levels of the drug peak after 3 to 4 hours, with a mean half-life ranging from 5 to 9 hours in young individuals, and from 11 to 13 hours in the elderly [22]. The main route of excretion is renal, but the drug is also expelled via the faecal/biliar route [23]. Rivaroxaban can be administered at a fixed dose in any patient and does not need laboratory monitoring. Also rivaroxaban has been licensed in the European Union and in Canada for the prevention of VTE in patients undergoing hip- and knee-replacement surgery, with a recommended dose of 10 mg once daily [24].
Two phase II, dose-finding studies compared rivaroxaban administered at total daily doses ranging from 20 mg to 60 mg with standard therapy with LMWH followed by oral vitamin K antagonists [25, 26]. Based on the positive results of these studies, the following doses were selected for further investigation in the three phase III clinical trials aimed to assess the acute phase and the long term treatment of DVT and PE (the Einstein studies): 15 mg bid for 3 weeks followed by 20 mg qd in the ongoing Einstein DVT and Einstein PE studies, in which patients with objectively confirmed, symptomatic DVT or PE are randomized to treatment with rivaroxaban alone or with LMWH and vitamin K antagonists for a total period of 3 to 12 months, and 20 mg qd in the Einstein Extension study, in which patients who had completed 6 to 12 months of anticoagulant treatment with either vitamin K antagonists or rivaroxaban (if also enrolled in the acute phase studies) after an acute episode of VTE were randomized to rivaroxaban or placebo for additional 6 to 12 months. The Einstein Extension study is already completed, and the results have been presented at the American Society of Hematology meeting in December 2009 [27]. In this randomised, double blind, placebo-controlled study, the primary efficacy outcome was the recurrence of symptomatic VTE and the principal safety outcome was the occurrence of major bleeding. During treatment, symptomatic recurrent VTE events occurred in 7.1% patients treated with placebo and in 1.3% patients treated with rivaroxaban (hazard ratio, 0.18; 95% confindence interval, 0.09-0.39). After stopping the study medication, 1.0% symptomatic recurrent VTE events occurred in both groups during the one month observational period of follow up. No major bleeding events were documented in the group of patients treated with placebo, 4 (0.7%) major bleeding events occurred in the rivaroxaban group (P =0.106). None of these bleeding events were fatal or occurred in a critical site. Clinically relevant non-major bleeding occurred in 1.2% and in 5.4% patients randomized to placebo and rivaroxaban, respectively. Two (0.3%) patients in the placebo group and 1 (0.2%) patient in the rivaroxaban group died.
Apixaban is an oral active Factor Xa inhibitor derived from razaxaban (an aminobenzisoxazole that binds to the active site of Factor Xa with high affinity), with superior pharmacological proprieties [17]. It is a small molecule able to inhibit in a selective and reversible manner the active site of both free and prothrombinase-bound Factor Xa. Preclinical studies demonstrate that apixaban has an oral bioavailability of more than 50%: its plasma peak is achieved in about 3 h and its half-life is about 12 h [28]. The drug is absorbed in the gastrointestinal tract, is metabolised in the liver by cythocrome-dependent and -independent mechanisms and it is eliminated through both the renal and the faecal routes [29].
Apixaban has been assessed for the treatment of DVT in a dose finding study (Botticelli DVT study) [30]. Patients were randomised to receive apixaban 5 mg bid, 10 mg bid, 20 mg od or LMWH vitamin K antagonists. The primary efficacy outcome, defined as the composite of symptomatic recurrent VTE and asymptomatic deterioration in the thrombotic burden as assessed by repeat bilateral compression ultrasonography and perfusion lung scan, occurred in 4.7% of patients treated with apixaban and in 4.2% of LMWH/vitamin K antagonists treated patients. No dose effect was observed across apixaban doses. The principal safety outcome, defined as the composite of major and clinically relevant non-major bleeding, occurred in 7.3% of the apixaban treated patients and in 7.9% of LMWH/vitamin K antagonists treated patients. On the basis of this study, phase III studies (AMPLIFY and AMPLIFY extension), testing apixaban at the doses of 10 mg and 5 mg twice daily, are now undergoing. Studies assessing the efficacy and safety of other factor Xa inhibitors, such as edoxaban, are also underway.
CONCLUSIONS
The current management of VTE is largely based on the use of anticoagulant drugs, both parenteral drugs such as UFH, LMWH or fondaparinux for the treatment of the acute phase and oral drugs such as the vitamin K antagonists for the long term secondary prevention. All these drugs have been proven to be highly effective in preventing thrombus propagation, embolization, and recurrence. For the management of the acute phase of the disease, LMWH has largely replaced UFH thus contributing to simplify the management of VTE, and now a large proportion of patients with DVT do not need to be hospitalized and can be entirely treated as outpatients. For the long term secondary prevention, vitamin K antagonists remain the only choice for clinicians, and their clear benefits in terms of efficacy need to be periodically balanced in each patient against their risks in terms of safety and their inconvenient management. In a very near future, the armamentarium of clinicians involved in the prevention and treatment of thromboembolic disorders could become much larger. After the positive results of the first clinical trials, new direct thrombin inhibitors and direct Factor Xa inhibitors that are administered orally are closely approaching the market. With predictable anticoagulant responses and low potential for food-drug and drug-drug interactions, these new agents can be given in fixed doses without coagulation monitoring. These properties and the oral administration render these compounds more convenient than both vitamin K antagonists and LMWH. Based on design of the phase III clinical trials, we can speculate that some of these compounds will challenge the vitamin K antagonists for the long term secondary prevention of VTE, and that other will also challenge the parenteral drugs for the acute phase management, as they are tested as a stand-alone treatment for both DVT and PE. Thus, patients with VTE could be treated with a single oral agent right after the objective diagnosis of the disease. Specific areas of particular interest for these new agents include the treatment of patients with cancer and VTE, for whom long term treatment with LMWH is currently recommended and for whom an oral agent with a low propensity for drug-drug interactions could represent the ideal therapy, and of course the long term treatment of patients with unprovoked VTE, where the complex balance between benefits and risks of the currently available drugs could be simplified with the use of more practical agents.
 XML Download
XML Download