

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
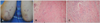
A 40-year-old male presented with 4 months history of multiple various sized erythematous to violaceous subcutaneous nodules on both extensor surfaces of elbows, which was partially movable and showed no symptoms (Fig. 1A). He was diagnosed as rheumatoid arthritis (RA) 7 years ago. A variety of therapeutic options, such as systemic corticosteroid, antimalarial drug, nonsteroidal anti-inflammatory drugs (NSAIDs), and methotrexate, were prescribed to control RA activity. However, they all failed to show symptomatic improvement. After that, the patient started adalimumab, a human monoclonal antibody to tumor necrosis factor (TNF)-α, 40 mg injection every other week with concomitant systemic corticosteroid, methotrexate and a NSAID. Adalimumab injection improved signs and symptoms of RA gradually. However, the multiple subcutaneous nodules occurred in the extensor sides of the elbows two months after adalimumab injection. A skin biopsy was performed and it showed dense fibrinoid deposits in deep dermis. At high magnification, large palisading granulomas surrounding degenerated connective tissue and fibrin were noticed and infiltrating inflammatory cells were mostly composed of lymphocytes and histiocytes. Mucin deposition was rarely observed. Overall, it was consistent with rheumatoid nodule (Fig. 1B, C). The patient didn't receive any treatment, and there was no change in the lesion at the follow-up visit.
Rheumatoid nodule development is extremely rare side effect of TNF-α antagonists and only two cases after etanercept and adalimumab injection have reported so far. However, in the previous report caused by adalimumab injection, rheumatoid nodule was diagnosed by only ultrasonogram1. Thus, to our knowledge, this is the first report of rheumatoid nodules confirmed by histopathologic diagnosis following the treatment with adalimumab.
Rheumatoid nodules are one of the most common extra-articular manifestations of RA, usually associated with severe disease activity. Macrophage is the main infiltrating inflammatory cell in both rheumatoid nodule and synovial membrane of RA and they show similar expressions of proinflammatory cytokines such as TNF-α, and interleukin-1 receptor antagonist (IL-1Ra)2. However, in this case, rheumatoid nodules were developed when the signs and symptoms of RA had been gradually improving by the adalimumab.
There are several differences between rheumatoid nodule and synovial membrane of RA. Rheumatoid nodules lack infiltrating B cells, plasma cells, and organized lymphoid structures. In addition, E-selectin expression, IL-1 level are higher and TNF-α concentration is significantly lower in the rheumatoid nodule compared to the synovial membrane of RA3, which suggests that development of rheumatoid nodules might be less influenced by TNF-α. One study with TNF-α knockout mice demonstrated abnormally low TNF-α level might induce an exaggeration of the effects driven by other inflammatory mediators4. Therefore, it could be considered that excessive TNF-α suppression could induce the development of rheumatoid nodules.
Furthermore, anti-TNF-α treatments increase peripheral blood counts which are thought to be related to reduced cell traffic to the inflamed joint in RA5. Thus it is conceivable that these migratory cells infiltrate other inflamed tissues and form rheumatoid nodules.
So herein, we report a case with great interest which could be one of the example and supporting clinical evidence of the paradoxical effects of anti-TNF-α treatment.
 XML Download
XML Download