

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic urticaria (CU) is defined as recurrent episodes of wheals for at least 6 weeks. CU is a common disorder with an estimated prevalence of 0.5% to 5% in the general population1. Although there are several known causes of CU, including physical stimuli, allergy, systemic illness, drug or infection, no definitive cause of CU can be identified despite a thorough medical evaluation in 80%~90% of cases2.
Since the 1980s, an increasing number of reports have suggested an association of CU with autoimmune disease. The presence of a serum factor that induced an immediate wheal-and-flare response following the intradermal injection of autologous serum from 44%~58% of patients with CU has been reported and the presence of autoantibodies capable of inducing mast cell degranulation was noted34. In the 1990s, studies demonstrated the presence of immunoglobulin G (IgG) autoantibodies directed against the α subunit of the high-affinity IgE receptor5 and autoantibodies directed against IgE6 in sera from 45%~55% of patients with CU. These autoantibodies have been shown to activate blood basophils and cutaneous mast cells, resulting in the release of histamine and other proinflammatory mediators7.
The association between CU and various autoimmune disorders, including thyroid disease, rheumatoid arthritis, systemic lupus erythematosus, Sjogren's syndrome, and type 1 diabetes has been recognized as indirect evidence of an autoimmune entity of CU8. Among them, autoimmune thyroid diseases were the most commonly reported autoimmune diseases in patients with CU9. Thyroid autoantibodies, indicators for the diagnosis of autoimmune thyroid disease, were found in 12%~37% of patients with CU1011. The role of thyroid autoantibodies in the pathogenesis of CU is debatable12. Several studies have suggested that epitopic cross-reactivity between thyroid autoantibodies and other autoantibodies found in CU lack evidence and thyroid autoantibodies themselves have no in vivo effect on mast cell and basophil releasability1314.
After a high prevalence of thyroid autoantibodies in patients with CU was reported, resolution of urticarial after thyroid hormone replacement therapy in some patients with concomitant thyroid autoimmunity was reported15, and some authors have subsequently recommended the therapeutic use of thyroid hormone in patients with CU16. However, to our knowledge, no studies have investigated the clinical response of urticaria to the treatment of coexisting thyroid diseases in a Korean population. In this study, we investigated the clinical response of urticaria to the treatment of thyroid dysfunction in Korean patients with CU.
MATERIALS AND METHODS
We retrospectively reviewed the records of patients with CU seen at the Department of Dermatology or Allergy & Clinical Immunology at Dongguk University Ilsan Hospital (Goyang, Korea) from July 2005 to June 2013. The diagnosis of CU was established by the presence of intermittent or continuous wheals for at least 6 weeks. Patients were excluded if they had primarily physical urticaria, food or drug-related urticaria, or urticaria vasculitis.
Demographic data and laboratory data were collected. Serum-free T4 (FT4) (normal, 0.93~1.70 ng/dl), thyroid-stimulating hormone (TSH) (normal, 0.27~4.20 µU/ml), anti-thyroperoxidase (TPO) (normal, 0~34.00 IU/dl), and anti-thyroglobulin (TG) (normal, 0~115.00 IU/dl) antibody levels were measured by an electrochemiluminescence immunoassay. Hypothyroidism was diagnosed by laboratory criteria of FT4 <0.9 ng/dl and TSH >4.2 µU/ml. Patients were classified as having subclinical hypothyroidism if they had a normal FT4 level, but had an elevated TSH level17. Hyperthyroidism was diagnosed by laboratory criteria of FT4 >1.70 ng/dl and TSH <0.27 µU/ml. All patients with thyroid dysfunction were examined by an endocrinologist. The clinical course of urticaria was reviewed in accordance with thyroid function. The clinical effectiveness of levothyroxine (or anti-thyroid drugs) in CU patients was defined as elimination of daily spontaneous wheals or a significant reduction of medication to control daily spontaneous wheals14. The clinical response of urticaria was evaluated until the normalization of thyroid function after treatment with levothyroxine (or anti-thyroid drugs).
Data was analyzed using PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA). Statistical significance was assessed using the chi-square test and p-values<0.05 were considered statistically significant.
RESULTS
Patient characteristics
In total, 184 patients with CU were enrolled in the study, with a mean age of 37.8 years (range, 12~72 years). Of the 184 patients, 56 were men (mean age, 37.8 years; range, 12~72 years) and 128 were women (mean age, 37.8 years; range, 12~68 years). All patients reported symptoms of CU for a mean duration of 14.6 months (range, 2 months to 30 years).
Thyroid autoantibodies and other laboratory findings
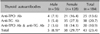
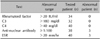
Thyroid autoantibodies (anti-TPO and/or anti-TG) were detected in 43 patients (23.4%) (5 men, 38 women). Of the 43 patients, 25 had increased levels of anti-TPO antibody, 38 had increased levels of anti-TG antibody, and 20 had increased levels of both anti-TPO and anti-TG antibodies (Table 1). The frequency of thyroid autoantibodies in women (29.7%, 38/128) was significantly higher than that in men (8.9%, 5/56) (p=0.002) (Table 1). In patients with thyroid autoantibodies, immunologic and other laboratory testing was not significant (Table 2). Rheumatoid factor, as well as complement C3 and C4, were normal in all patients. Erythrocyte sedimentation rate was elevated in three patients. Three patients had a persistent titer of anti-nuclear antibody ≥1:100 with no other evidence of connective tissue disorder.
Thyroid function
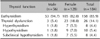
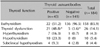
Of the total 184 patients with CU, 26 patients (14.1%) were found to have thyroid dysfunction (3 men, 23 women) and the remaining 158 patients (85.9%) were euthyroid. Of the 26 patients with thyroid dysfunction, eight were hyperthyroidic, 10 were hypothyroidic, and eight were classified as having subclinical hypothyroidism (Table 3). The frequency of thyroid dysfunction in women (18.0%, 23/128) was significantly higher than that in men (5.4%, 3/56) (p=0.024) (Table 3). The frequency of thyroid dysfunction in patients with thyroid autoantibodies (48.8%, 21/43) was significantly higher than that in patients without thyroid autoantibodies (3.6%, 5/141) (p<0.001) (Table 4).
Clinical response of urticaria to the treatment of thyroid dysfunction
Of the eight patients with hyperthyroidism, five were diagnosed with Graves' disease and treated with methimazole (3 patients) or propylthiouracil (2 patients). Although thyroid hormone levels were normalized after treatment with anti-thyroid drugs, none of the five patients showed any improvement of their respective urticaria. All 10 patients with hypothyroidism were diagnosed with Hashimoto's thyroiditis and treated with levothyroxine. As TSH levels decreased after treatment with levothyroxine, two of the 10 patients with Hashimoto's thyroiditis showed improvement in their urticaria (Table 5). All eight patients with subclinical hypothyroidism were not treated with levothyroxine, but were given repeated thyroid function tests due to the probability of developing a thyroid dysfunction. None of the eight patients with subclinical hypothyroidism experienced remission of urticaria during the follow-up period.
DISCUSSION
Thyroid autoimmunity is characterized by the formation of thyroid autoantibodies. Thyroid autoantibodies, indicators for the diagnosis of autoimmune thyroid disease, were found in 3%~9% of the general population, with the prevalence increasing markedly in women above the age of 45 years18. The prevalence of thyroid autoantibodies in the general Korean population was reported to be 8.9%19. In this study, we detected thyroid autoantibodies in 23.4% of patients with CU. This result is consistent with previous reports in which thyroid autoantibodies were found in 12%~37% of CU patients (Table 6)10111617202122232425. Our study showed that the prevalence of thyroid autoantibodies was significantly (p<0.05) higher in Korean patients with CU than the assumed prevalence (less than 9%) in the general Korean population.
The clinical presentation of thyroid autoimmunity varies from hypothyroidism in Hashimoto's thyroiditis to hyperthyroidism in Graves' disease. Hypothyroidism or subclinical hypothyroidism is more frequent than hyperthyroidism in patients with CU26. In this study, the prevalence of hyperthyroidism, hypothyroidism, and subclinical hypothyroidism in patients with CU was 4.3% (men 1.8%, women 5.5%), 5.4% (men 1.8%, women 7.0%), and 4.3% (men 1.8%, women 5.5%), respectively. The prevalence of hyperthyroidism, hypothyroidism, and subclinical hypothyroidism in the general Korean population has been reported to be 0.6% (men 0.4%, women 0.8%), 0.3% (men 0.1%, women 0.5%), and 1.8% (men 1.1%, women 2.7%), respectively27. Although it is difficult to compare the prevalence of thyroid dysfunction reported by different groups due to the differences in the study population, our data showed a high prevalence of thyroid dysfunction in patients with CU. The incidence of thyroid dysfunction has been reported as 12%~29% in CU patients and 24%~55% in thyroid antibody-positive patients with CU (Table 7)17202829. Our results confirmed these previous studies showing that thyroid dysfunction was present in 14.1% of patients with CU and that the prevalence increased to 48.8% if CU was accompanied by thyroid autoantibodies.
In this study, two of the 10 patients with Hashimoto's thyroiditis showed improved urticaria after treatment with levothyroxine, whereas none of five patients with Graves' disease showed any improvement of urticaria after treatment with anti-thyroid drugs. While the remission of urticaria after treatment with anti-thyroid drugs in patients with Graves' disease has been reported in only a few anecdotal cases, the resolution of urticaria after levothyroxine treatment in patients with Hashimoto's thyroiditis has been reported by several authors (Table 8)151630313233. Although treatment of thyroid dysfunction was effective in a minority of patients with CU, the results suggest a causal relationship between CU and thyroid autoimmunity. The underlying mechanisms by which anti-thyroid drugs alleviate urticaria remains unknown. However, levothyroxine therapy has been suggested to improve urticaria in patients with Hashimoto's thyroiditis14. There is evidence for a relationship between the degree of inflammation in the thyroid and the presence of urticaria34. Rumbyrt et al.14 proposed that an inflammatory response in the thyroid gland leads to a generalized inflammatory state and lowers the threshold of mast cells to other stimuli and Aversano et al.32 hypothesized that TSH might drive the production of proinflammatory cytokines and can regulate the immune response. According to these hypotheses, levothyroxine therapy would reduce the inflammatory response by TSH suppression and thus reduce the symptoms of urticaria35. These hypotheses remain unproven.
While the present study has limitations owing to its retrospective design with a potential of selection bias, it provides important information about the prevalence of thyroid autoantibodies and thyroid dysfunction in Korean CU patients. Although treatment of thyroid dysfunction was effective only in a minority of patients with CU (two of the 10 patients with Hashimoto's thyroiditis), the association with thyroid autoimmunity must be considered in patients with CU. Further studies are needed to determine the effect of thyroid hormones on CU.




 XML Download
XML Download