

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pruritus is a challenging symptom associated with various skin disorders. The consequent loss of sleep, physical disfigurement and skin lesions can even result in impairment of health-related quality of life. Skin senescence associated with skin dryness during old age causes long-term pruritus. Severe pruritus remains a difficult condition to control despite development in many treatment modalities. In addition, older patients have many limitations in using oral medication due to their underlying diseases and the possible interactions with the medications that they are already taking.
One of the main mediators that produce the itching sensation is histamine, which is induced by many other mediators, thus increasing histamine-induced pruritus. However, often, an antihistamine agent cannot effectively suppress all types of pruritus because some neuropeptides, proteases, and cytokines induce pruritus through a histamine-independent pathway.
The role of opiate receptors in the perception of pruritus is emphasized by the observation that opiate antagonists suppress pruritus of a different origin by modifying the neuronal sensation of itching1.
This study was designed to evaluate the efficacy and safety of naltrexone in the treatment of severe pruritus resistant to antihistamine agents in older patients.
MATERIALS AND METHODS
Sixteen patients with antihistamine-resistant severe pruritus were enrolled (Table 1) in this observational study. Informed consent was obtained from all patients, and the protocols were approved by the institutional review board (IRB No. 4-2011-0423). To study the safety and efficacy in older people, only patients 65 years and older with severe pruritus (a visual analogue scale [VAS] score 7 or higher) could sign up for the study. In addition, as naltrexone is not the first-line treatment option for pruritus, patients with a symptom that has not been easily controlled with conventional antipruritic medications were selected for this study. The mean age of the patients was 73 years (range, 65 to 83 years), and the men-to-women ratio was 6:4. Patients received 50 mg of naltrexone per day (Revia®; Bristol-Myers Squibb, Mulgrave, VIC, Australia) for approximately 2 months (average, 66.5 days), and were instructed to continue their previous therapies including systemic corticosteroids, phototherapies, extra antipruritics, topical corticosteroids, and emollients. Most of the patients were given naltrexone with antihistamines and topical agents. All the patients had persistent itching sensation, either generalized or localized, caused by prurigo nodularis, cholestatic pruritus due to cholestatic liver disease, uremic pruritus, eczema senilis, and cutaneous lymphoma. Some of the patients had pruritus of unknown origin. Baseline laboratory tests were performed on the first visit, including complete blood cell count and routine chemistry with liver function test. Efficacy was assessed with a VAS ranging from 0 (no pruritus) to 10 (the most intensive pruritus they can imagine)2 and scored at the beginning, after 2 weeks, and at the end of the 2-month naltrexone treatment. Additional evaluation was performed to check adverse drug effects. Statistical analysis was conducted through a paired t-test by using IBM Statistical Package for the Social Sciences Statistics ver. 21 (IBM Co., Armonk, NY, USA).
RESULTS
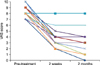
According to the VAS scores, 13 (72.2%) of 18 patients reported a "much improved" condition, experiencing more than 50% reduction in pruritus intensity (Table 1, Fig. 1). Among them, 6 (33.3%) reported an almost complete elimination of pruritus, with a VAS score of 0 or 1. Sixteen (88.9%) of 18 patients showed symptomatic improvement, and only 2 (11.1%) had persistent pruritus. The initial mean VAS score was 8.28±0.89, and at the end of the second week, the mean VAS score significantly decreased to 3.72±1.49 (p<0.05). Finally, at the end of 2 months, the mean VAS score was again significantly lower (2.83±1.98), compared with both the initial VAS score and the VAS score at the end of the second week (p<0.05). In terms of disease entities of pruritic skin disorders, patients with prurigo nodularis, cholestatic pruritus due to liver disease, uremic pruritus, xerotic eczema, eczema senilis, cutaneous lymphoma, and pruritus of unknown origin appeared to respond well to naltrexone. However, there was no statistically significant difference in drug efficacy related to the cause of pruritus (p=0.507). The first relief from pruritus was observed within 2 weeks, and the therapeutic effect was maintained during the study in all the patients who responded to naltrexone. In 14 (77.8%) patients, the first relief from pruritus was observed within a week. Five patients had side effects including insomnia (two patients), fatigue, constipation, and anorexia. Except for constipation, adverse reactions were restricted to the first 2 weeks, and constipation was well managed by laxatives. No patient exhibited any elevation in liver enzyme in the blood test or experienced deterioration of their underlying diseases.
DISCUSSION
Antihistamines are widely used to control pruritus, and they have been considered as the only antipruritic therapy that is available for various types of pruritus3. They are also generally safe for older patients, without causing considerable drug interactions. Many elderly patients benefit from antihistamines because they are usually already taking many other medications due to their underlying diseases. Yet, there are many pruritic conditions that cannot be controlled by antihistamines alone. In addition, histamine is not the sole cause of itching.
We used naltrexone (Revia®) as a second-line treatment option for older patients with severe pruritus that could not be controlled by other means. The result showed that naltrexone relieves pruritus from various skin diseases and even itchiness associated with an internal disease, without significant side effects in older patients. The symptom was significantly improved after 2 weeks of naltrexone treatment. The decrease in the VAS score at the end of 2 months was less prominent when compared with the VAS score reduction in the first two weeks. And yet it was also statistically significant. In addition, the overall decline in the VAS score in terms of significant pruritus improvement was observed at the end of the study (p<0.05). Side effects including insomnia, tiredness, and anorexia were limited to the first 2 weeks only, and constipation was managed with laxatives, revealing the safety of using naltrexone in older patients. Throughout the rest of the 2-month naltrexone treatment, no additional side effects were reported. Nausea is one of the most common adverse effects of naltrexone, and there was a report showing that younger patients are more likely to experience nausea4. Interestingly, none of our older patients had nausea. In our study with older patients, adverse reactions were reported in 5 (27.8%) patients. Other literature reported 11.1% to 38.5% of subjects with heterogeneous age and side effects reported throughout the treatment period567. In comparison with current literatures, naltrexone did not show a significantly higher frequency of side effects in patients who are older than 65 years.
It has already been reported that endogenous or exogenous opioids can induce or intensify pruritus8910. There is a general agreement on the fact that opioids induce an analgesic effect often in combination with pruritus evocation. However, a recent study showed that a long-lasting morphine-induced itch via µ-opioid receptor (MOR1) and morphine-induced analgesia occur independently, whereas short-acting morphine-induced scratching was provoked via isoform D of MOR1, and they are located on different sets of neurons8. The mode of action in the provocation of itch differs between central and peripheral applications91011. Opioid agonists themselves do not cause local itching upon injection or intradermal application. The antipruritic effect of MOR1 antagonists showed a central effect, and the κ-opioid receptor agonists revealed an effect on the spinal cord level. Opioid peptides have been implicated as mediators of cholestatic pruritus or pruritus of chronic kidney disease1213, and upregulation of MOR1 in atopic dermatitis has been reported as well14.
Several randomized controlled trials have reported significant improvement in pruritus by using naltrexone in cholestatic pruritus, chronic urticaria, and atopic dermatitis515161718, and a comparative study showed the efficacy of naltrexone in uremic pruritus6. The mean age of patients ranged from 45.3 to 62.6 years, and the study of Malekzad et al.5 had the most heterogeneous patient age, ranging from 24 to 85 years.
The antipruritic effect of naltrexone, a MOR1 antagonist, can be explained by a neuronal mechanism13. Administration of MOR1 antagonists inhibits pruritus by reversing the effect of opioids. Both pain-transmitting and pruritoceptive dorsal horn neurons run parallel to each other in the dorsal horn of the spinal cord, connected by opioid-sensitive interneurons. Usually, opioids act on pain-transmitting neurons and interneurons, producing neuronal inactivity and analgesia. Thus, the inhibition of interneurons on the pruriceptive neurons is repealed, clinically stimulating the itching sensation. Naltrexone inhibits the activation of MOR1 and suppresses itching.
Naltrexone is a synthetic congener of oxymorphone that blocks the effects of opioids twice as much as naloxone. Naltrexone displaces endorphins at the µ- and κ-receptors and exhibits minimal pharmacological activity. Additionally, naltrexone has great oral bioavailability and shows linear increase in the area under plasma concentration-time curve19. It is only contraindicated in patients with acute hepatitis, liver failure, and severe liver insufficiency and should not be used in children, pregnant, or breast-feeding women13. Moreover, it must not be given to persons with drug addiction or to patients who are taking opioid analgesics and opioid-containing medications. Naltrexone does not have abuse potential because it does not cause physical dependence. In addition, it appears to have a favorable risk-to-benefit ratio and is usually well tolerated. Common side effects of naltrexone include withdrawal-like reactions; gastrointestinal effects including nausea, vomiting, and diarrhea; cardiovascular effects including dizziness; and neurologic effects including fatigue and headache71516192021. However, they are generally limited to the first 2 weeks of treatment. As the effect of the drug usually manifests within 2 weeks, naltrexone could be challenged for the first 2 weeks and maintained on patients who respond to the medication.
The limitation of this study is the relatively small number of patients without an additional double-blind placebo group. Nevertheless, as it has already been proven that naltrexone could be an effective second-line option to treat pruritus, and as there has been no study on its use on older patients, we focused on the safety of using naltrexone for 2 months as well as on its efficacy in elderly patients.
In addition, old people tend to have more severe and long-standing pruritus than younger subjects due to concurrent xerosis and skin barrier impairment secondary to skin aging, making them harder to treat. The fact that older patients are vulnerable to pruritus emphasizes the value of efficacy of naltrexone in this study.
In conclusion, naltrexone should be considered a safe and effective alternative treatment for older patients with severe pruritus.

 XML Download
XML Download