

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Eccrine poromas are common benign cutaneous appendage tumors and generally arise in the middle-aged or elderly of either gender. Eccrine poromas occur as a solitary, slowly-growing, skin-colored, or pigmented (sometimes bright red), pruritic or painful, pedunculated, sessile papule or nodule, situated mostly on the soles or sides of the feet. Eccrine poromas have rarely been reported to occur on the postauriaular area1 and there has been only one such report2 in the Korean literature. Herein, we report a case of an eccrine poroma developing at a rare site (the postauricular area), which might have been misdiagnosed as epidermal cyst or trichofolliculoma.
CASE REPORT
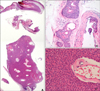
A 55-year-old Korean male presented with a mass on the right postauricular area for the last 10 years. The mass had gradually increased in size, and was not associated with pain or discharge. The examination revealed a solitary, 1×1 cm, protruding, dome-shaped, glistening, skin-colored-to-black mass (Fig. 1). Epidermal cyst or trichofolliculoma was considered in differential diagnosis. There was no previous history of trauma to the area. Histopathologic findings showed a tumor in the epidermis comprised of broad anastomosing bands with a sharp demarcation from the stroma (Fig. 2A). Narrow ductal lumina were found within the tumor. They were lined by a single row of the luminal cells covered by an eosinophilic lining (Fig. 2B). The tumor cells were smaller than epidermal keratinocytes and showed a uniform cuboidal appearance with a deeply-basophilic, round nucleus. They were connected by intercellular bridges (Fig. 2C). The diagnosis was confirmed by histopathologic findings as an eccrine poroma. The tumor was excised and no recurrence was noted during the follow-up period of 5 months.
DISCUSSION
Because the eccrine poromas originate from the epidermal sweat duct unit, the distribution of eccrine poromas has corresponded to the density of sweat glands. The palm and sole have the highest densities of eccrine sweat glands, and indeed, the numerous reported cases of eccrine poromas were limited to those locations. However, eccrine poromas can develop on any part of the body where eccrine glands exist.
Hyman and Brownstein3 reviewed 45 new cases and 56 reported cases of eccrine poromas; 69 cases (68%) were located on the feet and the remaining 32% of tumors were on the calves, popliteal areas, knees, thighs, buttocks, hands, shoulders, abdomen, back, scalp, ears and neck, and the chest. Goldman et al.4 reported that the most common tumor sites were the soles of the feet (65%), followed by the hands (10%). Fourteen cases of eccrine poromas have been reported in the Korean literature. Seven cases involved the head and neck; among them, the most common sites were the scalp (4 cases) and face (temple and paranasal area), in descending order of frequency. Apparently, it is very rare to have any case of eccrine poroma located on the head, including the face. In this case, the tumor developed on the postauricular area, which is a rare location in that only one case2 has been reported in the Korean literature.
It has not been reported yet if there is any difference between poroma of the head and neck and extremity lesion clinically or histopathologically. According to Moore et al.5 that compared 10 cases of poroma of the head and neck with 10 cases of that of extremities, three cases of the latter exhibited clinical symptoms, such as pain, bleeding, a clear discharge, or a history of rapid growth, while none of the former showed any kind of symptoms. The symptoms in the lesions of the extremities could be related to trauma, particularly in those lesions on the weight-bearing portion of the foot. The group of the head and neck showed four times more of pigment, whereas, 25% of all cases of poroma had pigment. Horn cysts were 5 times more common in the lesions of the extremities.
One thing that deserves attention of clinicians is that correct pre-operative diagnosis was included in the differential diagnosis only for the lesions on the foot5. In the inappropriate belief that poromas are primarily acral lesions, clinical diagnosis is difficult, and lesions are often mistakenly identified as granuloma pyogenicum, nevus or fibroma. Since this case presented as a small, solitary, dome-shaped, skin-colored-to-black mass situated on the postauricular region, epidermal cyst or trichofolliculoma was suspected clinically. Trichofolliculoma was ruled out readily, as the tumor under discussion lacked a central, dilated, large, primary hair follicle lined by infundibular and isthmus type epithelium and numerous, smaller, secondary hair follicles radiating from the primary hair follicle. The tumor differed from an epidermal cyst by the lack of the cystic cavity containing abundant laminated orthokeratin and cyst wall consisting of a stratified squamous epithelium with a granular layer typically observed in epidermal cyst.
The histologic differential diagnosis should be made against the basal cell carcinoma and seborrheic keratosis. Poroma differs from the basal cell carcinoma by displaying a more organoid appearance; that is, fairly uniform anastomosing cords of epithelium, the uniformity of the cuboidal cells, and the general lack of peripheral palisading of the nuclei and separation artifact. In general, seborrheic keratosis of clonal type do not exhibit epithelial cells as small as those observed in poroma or the association with sweat ducts.
In this case, we managed a case of an eccrine poroma occuring on the postauricular area, which is considered a rare case, and which might have been misdiagnosed as an epidermal cyst or trichofolliculoma. Care should be taken to differentiate eccrine poromas from other dermatoses when they arise in areas other than the hands and feet.

 XML Download
XML Download