

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Digital mucous cysts (DMCs) were first described by Hyde1 in 1883 under the name of synovial lesions of the skin, with other names proposed, including myxoid cyst, mucinous cyst, mucoid cyst, and synovial cyst. It is clinically characterized by a round to oval, translucent, smooth nodule localized to the dorsum of the finger near the distal interphalangeal (DIP) joint2. It usually presents as a solitary lesion, and rarely, as multiple lesions. However, the herpetiform appearance of DMCs on one digit has not been reported in dermatologic literature.
CASE REPORT
An 88-year-old man presented with several round to oval dome shaped papules on his right thumb. The lesion first developed 2 years ago as a small solitary papule and subsequently several other papules developed around the first one. He had no past history of DMCs, osteoarthritis, or any other skin condition. Cutaneous examination revealed several grouped 2 to 3 mm round to oval translucent dome-shaped papules presenting as herpetiform lesions on the dorsum of his right thumb between the proximal nail fold and the DIP joint (Fig. 1). The remaining physical examination was unremarkable.
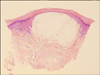
A punch biopsy was performed from one of the papules on his right thumb, and histopathology showed a cystic space containing mucinous material and a number of fibroblasts in the dermis (Fig. 2). The cystic space was surrounded by mucinous stroma and lining of the cyst wall was not apparent. Alcian blue (pH 2.5) staining was positive for mucin in the cystic spaces. From these findings, the diagnosis of a DMC was made. We recommended total excision of the lesion, but he declined treatment.
DISCUSSION
A DMC is solitary, translucent, round to oval, dome-shaped, skin-colored cystic nodular lesion on the digits of the hands2. It contains a clear gelatinous fluid that may discharge spontaneously or on minor trauma. It is usually located between the crease of the DIP joint on the dorsal surface and the proximal nail fold. Less commonly, it is found between the proximal nail fold and the nail plate, beneath the nail matrix, or in the digit pulp. Most cysts occur in people 40 to 70 years old, and women are affected more than twice as often as men3,4.
Two types of DMCs have been described. The first is the myxomatous type, which is analogous to focal mucinosis, and shows a large cystic space containing mucin surrounded by collagen fibers with no lining of the cyst wall. It results from an overproduction of hyaluronic acid by the fibroblasts, and it is not anatomically connected with the adjacent DIP joint2,5. Histologically, there are ill-defined areas of mucinous material in its early stages. Subsequently, multiple clefts form and then coalesce into one large cystic space containing mucin composed largely of hyaluronic acid. The collagen at the periphery of the cysts appears compressed. The second type is the ganglion type, which is associated with changes of degenerative joint disease and commonly seen in elderly patients with osteoarthritis and osteophytes. It results from herniation of the tendon sheath or joint linings, thus representing a ganglion6. The ganglion type shows evidence of a pedicle leading to the joint space, and may show an epithelial lining2. Methylene blue injection can identify communication between the cyst and DIP joint7. Both types of DMCs are characteristically present as a solitary lesion, and multiple lesions are rare. Our patient had herpetiform papules on his right thumb. Although there was no history of direct skin-to-skin contact, trauma, HSV infection, or HIV infection, we first diagnosed the lesion to be molluscum contagiosum or herpetic whitlow. Histopathology showed a cystic space containing mucinous material stained with Alcian blue (pH 2.5) and the lining of the cyst wall was not apparent. Therefore, we diagnosed the patient with the myxomatous type of DMCs.
Several cases of multiple DMCs have been reported in the dermatologic literature. Connolly and de Berker8 reported DMCs involving the fingers of both hands due to repetitive occupational trauma. Kivanc-Altunay et al.9 reported digital subungual mucous cysts on all toes. However, DMCs presenting as herpetiform lesions, as in our patient, have not been previously reported. Lack of awareness of its special clinical feature may contribute to erroneous diagnosis. Molluscum contagiosum, herpetic whitlow, and some benign tumors may be difficult to differentiate. Correct diagnosis can be confirmed by histopathology and radiological exam like ultrasonography and MRI.

 XML Download
XML Download