

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Oral zinc compounds have been used for decades for treating disorders such as telogen effluvium1,2 and alopecia areata3,4. Reports have also been published on oral zinc sulfate therapy with encouraging results for some cases of alopecia areata. In 1976 Wolowa and Jablonska5 reported that two patients with alopecia areata regrew their hair after treatment with oral zinc sulfate. It has been reported that some alopecia areata patients have zinc deficiency6-8. Zinc is an essential cofactor for multiple enzymes and it is involved with important functional activities in the hair follicle. Further, zinc is a potent inhibitor of hair follicle regression and it accelerates hair follicle recovery6,7. In the present study, we examined the serum levels of zinc in alopecia areata patients. We studied the therapeutic effect of 12 weeks oral zinc supplementation for treating alopecia areata patients who have a low serum zinc level and we checked their serum zinc level after this oral zinc supplementation.
MATERIALS AND METHODS
Patients
Forty four alopecia areata patients were checked for their serum zinc levels. After the zinc levels were checked, 15 alopecia areata patients who each had a low serum zinc level (Zn≤70 µg/dl) were enrolled in this study. Ten were males and five were females (mean age: 29.1±16.2 years). All of these patients had had alopecia areata for at least 6 months before visiting our clinic for treatment. These patients had reported no effect from other therapeutic methods or they had had no treatment history for more than 6 months before visiting our clinic. The sera obtained from the 15 alopecia areata patients were used as test materials.
Methods
Supplementation with oral zinc gluconate tablet (50 mg/tablet/day, zinc 50, GNC, USA) was used as a therapeutic method for twelve weeks without any other treatment. Each patient's serum zinc level was measured before and after supplementation therapy. We defined a mild type of alopecia areata as hair loss of less than 25% of the total scalp hair, a moderate type of alopecia areata was defined as hair loss between 25% and 50% of the total scalp hair and a severe type of alopecia areata was defined as hair loss of more than 50% of total scalp hair. The therapeutic effects of oral zinc supplementation in alopecia areata patients were evaluated through the extent of vellus hair and terminal hair regrowth on the scalp. We graded the therapeutic effects as follows:
(1) Marked recovery: cosmetic satisfaction or terminal hair regrowth of more than 60% on the hair loss patch
(2) Partial recovery: terminal hair regrowth less than 60% on the hair loss patch
(3) Poor recovery: only vellus hair regrowth on the hair loss patch
(4) No recovery: aggravation or an unchanged alopecia areata state as compared to before therapy
RESULTS
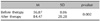
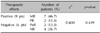
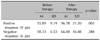
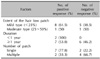
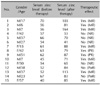
All of the 15 subjects completed this study. They were enrolled from September 2006 to August 2007. The patient information is shown in Table 1. After the zinc supplementation the mean serum zinc level changed from 56.9 µg/dl to 84.5 µg/dl. The results of the changed serum zinc levels are shown in Table 2, and the differences of the zinc serum levels were statistically significant before and after supplementation therapy (p=0.002). Positive therapeutic effects were seen in 9 out of 15 patients (66.7%). Out of the 9 patients with positive therapeutic effects, 7 patients showed a marked recovery (Fig. 1) and 2 patients showed a partial recovery. However, the therapeutic effects were not statistically significant (p=0.439, Table 3). After zinc supplementation, there was a difference of the serum zinc level between the positive response group and the negative response group. The serum zinc level of the positive response group increased by 40.9 µg/dl and that of the negative response group increased by 7.7 µg/dl. In the positive response group, the serum zinc levels after therapy were significantly higher than those before therapy (p=0.003). The changed serum zinc levels are shown in Table 4. The patients with mild alopecia areata and who had a single alopecia areata patch displayed more positive results than the patients who had multiple alopecia areata patches (Table 5). Two patients complained of mild nausea as a side effect. The summary of the patients is shown in Table 6.
DISCUSSION
There are several reports stating that the serum zinc level is low in alopecia areata patients7,11-13. However, the pathogenesis of this reduced serum zinc level is unknown. As cofactors of metalloenzymes, zinc has considerable effects on nearly all aspects of the metabolism that takes place in the organs of the body, including the skin. In fact, congenital and acquired zinc deficiencies are usually expressed as a variety of skin manifestations such as acrodermatitis enteropathica, psoriasis-like eruptions, blisters, onychopathy and loss of hair6,14. Several reports have shown that oral administration of zinc compounds improved hair growth5. Yet in 1981, Ead15 reported that oral administration of zinc compounds had no therapeutic effect on hair loss. Ead15 found that after zinc supplementation, the serum zinc level changed from 77.5 µg/dl to 112.2 µg/dl and the serum zinc level increased by 34.7 µg/dl, but the patients did not show a positive therapeutic effect. In this study, 6 out of 15 patients belonged to the negative response group. Among this negative response group, 4 patients' serum zinc levels increased and 2 patients' serum zinc levels decreased. We think that the increased serum zinc levels in the 4 patients are related to another cause. The serum zinc level of three patients except patient No. 12, increased less than those of the positive response group. We thought that the No.12 patient's cause of hair loss was related to stress and fatigue. Two patients with decreased serum zinc levels had an irregular oral zinc tablet intake during this study. Zinc is a metal moiety of many enzymes and it is indispensable for normal cellular function and it has important roles in bone formation, cell-mediated immunity, the general immunological defense of the host and tissue growth. Zinc provides structural integrity to enzymes and/or it participates directly in catalysis. Examples of zinc metalloenzymes include DNA and RNA nucleotidyl transferases, alcohol dehydrogenase, glutamic, lactic and malic dehydrogenase and δ-aminolevulinic acid dehydratase16. The etiology of alopecia areata is still unknown. Several kinds of treatments have been tried with various results, i.e., oral and topical corticosteroids, triamcinolone intralesional injection, photochemotherapy, topical irritants and allergens, immunosuppressants and cryotherapy. Checking the serum zinc level is necessary to evaluate hair loss of an unknown cause, and zinc supplementation may be needed in the alopecia areata patients who have a low serum zinc level. In this study, after adhering to zinc supplementation for twelve weeks, the patients' mean serum zinc level changed from 56.9 µg/dl to 84.5 µg/dl, and the level increased by 27.60 µg/dl. When analyzing the differences between the positive and negative response groups, the positive response group increased their serum zinc level by 40.9 µg/dl, and the negative response group increased their serum zinc level by 7.7 µg/dl. This difference was statistically significant. Those patients with mild alopecia areata and those with a single alopecia areata patch had a greater positive response than the patients with moderate alopecia areata and those with multiple alopecia areata patches. The positive response group maintained zinc supplementation for at least 6 months with no recurrence of their hair loss being seen during their follow-up. The positive response group also showed continuous terminal hair regrowth during follow-up. Although these patients had a mild type of long term alopecia areata, zinc supplementation can become a possible adjuvant therapy when combined with other therapeutic methods, and especially for those alopecia areata patients with a low serum zinc level. Prior to this study, there has only been one report of alopecia areata patients having a low serum zinc level in the Korean medical literature3 and there has been no report about the therapeutic effects of zinc supplementation in Korea. This study was the first in Korea to evaluate the therapeutic effects of twelve weeks of oral zinc supplementation in alopecia areata patients with a low serum zinc level and we reported on the changing serum zinc levels after oral zinc supplementation. Positive therapeutic effects were seen in 9 out of 15 patients, but because of the small numbers of patients, the therapeutic effects were not statistically significant. Subsequent studies with a large number of alopecia areata patients are needed to clarify the therapeutic effects of oral zinc supplementation.


 XML Download
XML Download