

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Internet addiction (IA) is becoming a widespread and problematic phenomenon. The prevalence of IA has increased rapidly in East Asia. Additionally, younger and younger children are using the internet, which is a trend that has increased over the years. Internet users in China and the United States usually start surfing the internet from approximately 6 to 9 years old, and 62.7% of Korean users begin using the internet when they are between 3 and 5 years old [123]. The IA rates of children and youths have continuously increased, such that they were 7.3% for Korean children (5–9 years old) and 10.7% for teenagers (10–19 years old), which are higher than the rate of 6.8% of adults (30–49 years old) [3].
From the investigation of previous studies into individual factors that could influence childhood IA, self-control and self-esteem were suggested as important variables [45]. For school-aged children, their self-control and judgment is very poor for cognitive, psychological, and emotional growth when compared to adults or teenagers [6]. This can lead to various problems, such as difficulty in adjusting to school life; poor relationships with friends; insufficient communication with family members; the avoidance of interpersonal relationships; insufficient sleep; symptoms of depression, nervousness, hostility, fear and paranoia; and behavioral issues, such as violence and distraction [789].
Since IA has been increasingly recognized as a serious mental disorder, there have been several reviews addressing its causes, diagnosis, epidemiology, phenomenology, comorbid disorders, and neuroimaging findings. However, few studies have focused on the prevention and treatment of IA. There have been three meta-analyses investing the effects of the prevention or intervention treatment for IA. The effects of psychological and pharmacological interventions have been investigated for all ages [10]. The effects of group counseling programs have been analyzed for teenagers [11] and Oh and Kim [12] conducted a meta-analysis of teenagers in terms of the effects of a program of IA prevention and interventions. However, no study has produced clinical recommendations for school-aged children based on meta-analysis. Therefore, we conducted a meta-analysis to evaluate the available evidence of the effectiveness of various psychosocial interventions and to identify intervention moderators for IA in children. Potential moderating variables were determined based on previous research [101112] and methodological considerations. Type of intervention, approach, duration, grade, and setting were chosen as potential moderators.
II. Methods
1. Eligibility Criteria
The PICOTS-SD (participants, interventions, comparisons, outcomes, timing of outcome measurement, settings, study design) formulation was used to conduct a systematic review and meta-analysis to identify the scope of the literature on psychosocial interventions for IA.
1) Inclusion criteria
The participants were the general population of school-aged children. Types of interventions included psychosocial intervention defined as an intervention primarily designed to emphasize psychological or social factors rather than biological factors [13]. The main comparisons of interventions were usual care, no intervention, or a comparison intervention. The types of outcome measures were internet addiction, self-control, and self-esteem. The timing of outcome measurement was immediately after the psychosocial intervention or the follow-up period. The trial settings considered were both schools and community settings, such as community children centers. The study design included randomized controlled trials (RCT), non-randomized controlled trials (NRCT), and controlled before-after studies.
2) Exclusion criteria
Studies that met the following criteria were excluded (1) case studies, (2) studies where the full text was unavailable, (3) studies that provided insufficient data to perform an analysis of the effect sizes, and (4) studies that failed to report the results for at least one of the three outcome variables.
2. Search Procedure
With guidance from informatics experts, search strategies were applied from February 3 to March 30, 2015. Studies were identified by searching PubMed, the Cochrane Clinical Trial Library, EMBASE, CINAHL, NANET, DBpia, KSI KISS, KMbase, KoreaMed, NDSL, RISS, and KCI. Extensive searches were conducted for studies published between the first available year and January 2015 using the following search string: 'internet addiction OR internet usage OR problematic internet' AND 'psychosocial OR non-pharmacological OR behavior' AND 'treatment OR therapy OR program' AND 'child OR elementary students'. Unpublished data, conference proceedings, theses, and dissertations were included. We also conducted a manual review of relevant journals and of reference lists of relevant articles. Each search was limited to the English and Korean languages. Each identified article was further examined by two independent reviewers. Disagreements were resolved through discussion.
3. Quality Assessment
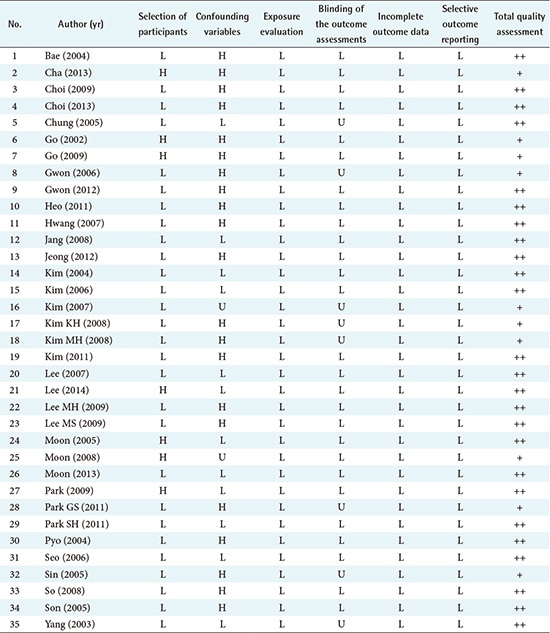
The methodological quality of the studies was evaluated using the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS) [14]. This tool consists of the following six domains: the selection of participants, confounding variables, the exposure evaluation, the blinding of the outcome assessments, incomplete outcome data, and selective outcome reporting. Individual domains were estimated as 'low risk of bias', 'unclear', or 'high risk of bias' by two authors who had experience with meta-analysis (Appendix 1).
4. Data Extraction
The following information was collected: author, publication year, study design, the country in which the study had been performed, school grade, total sample size, the number of participants in different groups, the type of treatment, approach, session, duration, hours of intervention, the type of control group, setting, mean and standard deviation of outcome variables, assessment tools, follow-up period, and study quality. In the case of two experimental groups, the data were extracted by dividing the individual studies.
5. Data Synthesis and Analysis
RevMan 5.3, a program of the Cochrane Library, calculated the meta-analysis of the effect size of an intervention. A Cochrane's chi-square test and Higgin's I2 were performed to determine the homogeneity of this study. When significant homogeneity (p > 0.1 and I2 < 50%) was present, a fixed-effects model was employed for pooled analysis. When significant heterogeneity (p ≤ 0.1 and I2 ≥ 50%) was present, a random-effects model was employed for pooled analysis. The statistical meaning of the effect size was decided by the whole effect test and a 95% confidence interval (CI), and it was based on a 5% significance level. The statistic created by this procedure is Cohen's d [15], of which an effect size of 0.20 is considered small, 0.5 is considered moderate, and 0.8 is considered large. The confidence verification for the calculated effect size was estimated using fail-safe numbers that examine whether the effect size calculated from the results of published studies so far is insignificantly affected by unpublished results. Because so few papers have been written on this topic, it could be concluded that the effect from the meta-analysis was reliable [16].
III. Results
1. Study Selection
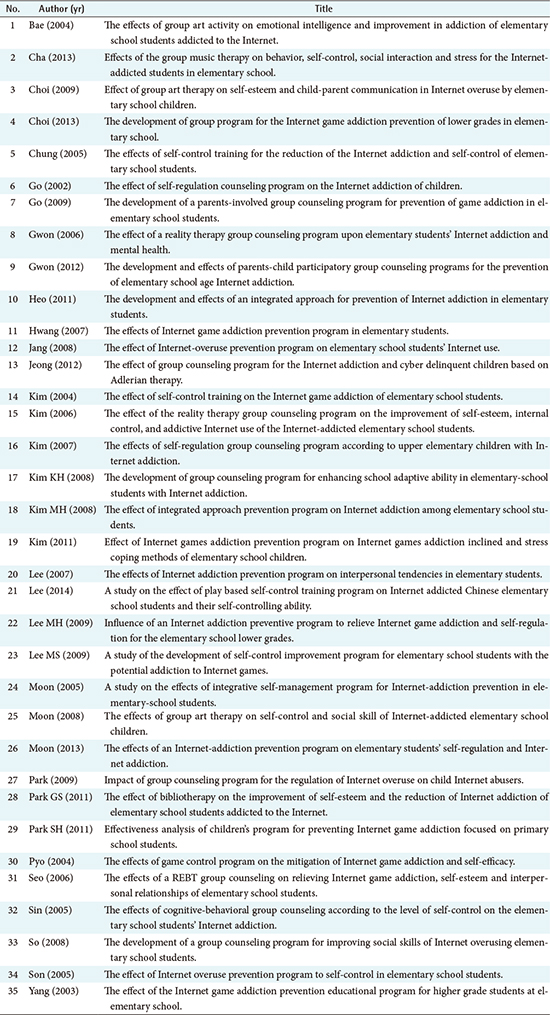
Figure 1 shows the study selection process. As a result of the first bibliographic search, a total of 3,421 papers were retrieved and 1,546 papers were selected by the removal of duplicates. Then, 138 papers were selected after confirmation that the titles and abstracts were applicable. Finally, 35 papers were selected for systematic review by confirmation of the full text. By the inclusion of 2 papers with two experimental groups, a total of 37 papers were selected for meta-analysis (Appendix 2).
2. Study Characteristics
The characteristics of the included studies are summarized in Table 1. Of the total 1,490 participants, the experimental group included 759 people, and the control group contained 731 people. The study design included 5 RCT studies and 32 NRCT studies.
3. Methodological Quality of the Intervention Studies
There was a high bias in seven of the studies in relation to the selection of participants, where participants were assigned to the intervention group or the control group. From the evaluation of confounding variables, 21 studies had high selection bias. Two studies were unclear in their reporting. For the blinding of the outcome assessments, 29 studies were considered to have a low bias risk because the blinding did not affect the measurement.
4. Effects of Interventions
1) Internet addiction
Thirty-six of the 37 included studies measured IA. The total population involved in these studies was 1,462. Psychosocial intervention applied to school-aged children had a large, statistically significant effect on the decrease of IA (standardized mean difference [SMD], –1.19; 95% CI, –1.52 to –0.87), and the overall heterogeneity was high (I2 = 86%) (Figure 2).
To identify the intervention moderators, further analyses were carried out. The types of intervention with a large effect on reducing IA were parent-involved counseling (SMD, –2.92; 95% CI, –4.30 to –1.54) and self-control training programs (SMD, –2.62; 95% CI, –4.07 to –1.17) (Figure 2). Even if both had a statistically significant effect, the selective approach (SMD, –1.54; 95% CI, –2.03 to –1.04) showed a larger effect than the universal approach (SMD, –0.78; 95% CI, –1.18 to –0.37). Comparing the effectiveness of the interventions based on their duration and grade, the programs consisting of more than 10 sessions (SMD, –1.59; 95% CI, –2.13 to –1.05) showed a significantly larger effect than the programs consisting of fewer than 10 sessions (SMD, –0.92; 95% CI, –1.30 to –0.53). The studies that targeted the upper grades (SMD, –1.25; 95% CI, –1.60 to –0.91) showed a statistically significant effect, but the studies that targeted the lower grades showed no statistically significant effect (SMD, –0.43; 95% CI, –0.88 to 0.02). The effect size at follow-up for the IA outcome variables was large and significant (SMD, –1.69; 95% CI, –2.73 to –0.65) (Table 2).
2) Self-control
Self-control was reported in 13 studies. The total number of participants available for analysis was 546. The analysis of these studies showed a small, statistically significant effect (SMD, 0.29; 95% CI, 0.11 to 0.47). The overall heterogeneity for the effects on self-control was high (I2 = 84%) (Figure 3).
The interventions with a large effect size on improving self-control were the self-control training program (SMD, 1.40; 95% CI, 0.81 to 1.99), and group counseling (SMD, 1.00; 95% CI, 0.48 to 1.52) (Figure 3). The interventions that used the selective approach showed a statistically significant improvement in self-control (SMD, 0.56; 95% CI, 0.29 to 0.84), while the universal preventive approach was not statistically significant (SMD, 0.10; 95% CI, –0.13 to 0.33). For improving self-control, the longer programs (SMD, 0.67; 95% CI, 0.22 to 1.11) had a larger effect than shorter programs (SMD, 0.22; 95% CI, 0.02 to 0.41) (Table 2). A subgroup analysis of grade and follow-up was considered. However, sufficient data were not provided for self-control.
3) Self-esteem
Six studies assessed the effects of psychosocial interventions on the level of self-esteem among school-aged children. The total number of participants was 142. Figure 4 shows that there was a large and statistically significant increase in the psychosocial intervention group when compared with the control group at the end of the intervention (mean difference, 3.58; 95% CI, 2.03 to 5.12). The overall inconsistency was at an acceptable level (I2 = 44%).
The interventions with a large effect were the integrated IA prevention program (mean difference, 7.25; 95% CI, 3.58 to 10.92) and reality therapy (mean difference, 4.29; 95% CI, 1.30 to 7.28) (Figure 4). Both of these approaches showed a large, statistically significant improvement in self-esteem (selective approach: mean difference, 2.92; 95% CI, 0.67 to 5.18; universal approach: mean difference, 4.51; 95% CI, 2.03 to 6.27). The studies with shorter interventions (mean difference, 4.20; 95% CI, 2.47 to 5.93) showed a statistically significant positive effect, while the longer interventions (mean difference, 1.12; 95% CI, –2.32 to 4.56) had no statistically significant effect. Only the self-esteem outcome provided appropriate data that could be used for analyzing the effect size by setting. The mean effect size of the studies conducted in a community child center (mean difference, 7.39; 95% CI, 3.85 to 10.94) was larger than that of the studies conducted in a school (mean difference, 2.68; 95% CI, 0.9 to 4.40) (Table 2). Grade and follow-up data for self-esteem were not available.
IV. Discussion
Even though IA has become a serious concern in modern society, research analyzing the effects of intervention to prevent or mitigate it is still lacking. This review found that psychosocial interventions have been beneficial for reducing IA and improving self-control and self-esteem at certain times. Self-control training programs, integrated IA prevention programs, and parents-involved counseling have had large and robust significant effects out of all of the outcome variables. The self-control training programs consisted of four components, such as self-consideration, environment planning, self-evaluation, and self-reinforcement [17]. Self-control training programs have been suggested by many experts to increase the effect of interventions in treating addiction [18]. They have also been reported to promote mental health [19]. Programs connected with various theoretical backgrounds, such as cognitive behavior therapy (CBT), music therapy, art therapy, reading therapy, time or stress management, and establishment of a coping plan were more effective than simple approaches [20]. Song and Park [21] identified the following items for IA programs based on the opinions of field experts: ability enhancement for self-control, social training enhancement, life goals and values establishment, support and intervention of family, promoting self-esteem or overcoming depression, and so on. Family-based interventions appear to be the most promising, not only with these outcomes but also for adolescent alcohol use [22] and depression symptoms in children and adolescents [23]. Due to limited studies verifying this approach, more studies are needed to assess the involvement of family members or other relatives in the treatment of IA.
All studies included in this analysis were developed for a group. Evidence suggests that group counseling appears to be the predominant modality for treating addiction. One advantage of a group program is its economical factor, because it targets many students simultaneously. In addition, the support, confrontation, and insight gained from other individuals experiencing similar recognition and emotions facilitate therapeutic recovery [24]. A previous study also mentioned that a group of less than 14 people showed more than a 90th percentile of effect size [12]. However, group therapy may not become truly beneficial until parents overcome the barriers associated with social anxiety, social isolation, and lack of social competence. Therefore, it is necessary to develop a program with appropriate methods for the participants' characteristics.
When interventions were analyzed according to the intervention purpose, trials with selective samples were more practicable and beneficial than those that target universal samples. A similar effect was found in a previous review [12]. However, it is possible that, although universal programs yield a low effect, they still could be cost-effective if they can prevent IA at comparatively low cost.
Regarding the effect of intervention according to duration, two-thirds of those studies reviewed had more than 10 intervention sessions. This group exhibited statistically significant effects for IA and self-esteem outcomes. A previous review of psychosocial interventions analyzing such outcomes as depression symptoms among older adults demonstrated that longer interventions showed statistically significant effects [19]. Likewise, this meta-analysis verified IA program interventions of more than seven sessions, which included more than a 90th percentile of effect size, for the target of adolescents [12]. Therefore, because a certain period is necessary to change the recognition and behaviors of participants, long-term programs might be more effective than short-term programs.
The results indicated that the pooled effect sizes for short-term efficacy for all outcomes were statically significant. However, many studies made it difficult to determine the long-term efficacy of the intervention because they failed to conduct a sufficiently long follow-up. Only nine studies reviewed here conducted a follow-up. To address this important topic, further research should consider long-term efficacy.
Another interesting result of our analysis was that 36 out of 37 studies were performed in South Korea, and one study was conducted in China. There were no studies available in the United States or Europe that investigated psychosocial intervention and its effect on the target of school-aged children. This reflects that the language was limited to English and Korean when the papers were extracted, but it can also be interpreted that IA is rapidly increasing in East Asia. Even from previous studies, 13 out of a total of 17 articles were published in South Korea and China, meaning that it was absolutely higher than for other regions [9]. Due to a lack of conclusive evidence of cultural differences in IA, further research is highly recommended in this area.
This study offers insight into the current state of psychosocial intervention programs for IA for the target population of school-aged children, and it is a first step in the development of evidence-based intervention recommendations. Nevertheless, a number of limitations should be noted. First, as fewer studies applied RCT, the confirmative evaluation results were not included for the effect size. As noted in a previous review [25], IA intervention studies tend to lack conformity, with inconsistencies in the definition and diagnosis of IA and a lack of randomization, and adequate comparison groups. The methodological weaknesses of the included studies are potentially a problem because a meta-analysis can only be as good as the studies upon which it is based [26]. Second, as the studies included in this analysis had high heterogeneity and there was a limited number of articles, sub-analyses on scale were not indicated. Scale selection with consideration of the characteristics of programs and subjects is necessary to identify the effects of IA improvement programs more precisely, and it can be considered that scales can verify the effect size if more articles are accumulated in the future.





 XML Download
XML Download