

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Provision of nursing services over the phone has grown significantly over the past two decades and are likely to continue to grow in the future in order to cut medical expenses. Telephone nursing is defined as all nursing services delivered over the telephone [1]. In telephone nursing, the patient usually makes a phone call to a nurse, then a nurse elicits or listens to the patient's concerns, provides support and information, or guides the patient to resources based on the concerns stated over the telephone [2-4]. Telephone nursing is used by various populations such as the chronically diseased, aging, pediatric and rural populations, and in various settings such as call centers, home health agencies, emergency centers, hospitals, primary care, and specialty clinics. Telephone nursing is different customer relationship management (CRM) following up with the patients for the purpose of retaining or preventing them from migrating to other hospitals.
Telephone nursing has been used to take care of early discharged patients since 2002, when seven diagnosis-related groups (DRGs) were introduced in Korea. One of the seven DRGs is senile cataract surgery, which is the most frequently performed surgery in Korea, making up 18% of all total surgeries [5]. Senile cataract patients who have received surgery leave hospital on the same day as the operation, unless they have complications from the surgery due to DRGs [6]. Consequently, many senile cataract surgery patients and their family members make phone calls to the nurse station to seek answers for questions and advice on the management of various problems arising at home. Before the introduction of DRGs, most of these problems were taken care of by the nurses during the patients' hospitalizations.
However, there is no guideline for nurses to follow for triage when providing care to a patient or family member over the phone. Telephone calls received by the ophthalmological nursing unit can be categorized as one of the following four types: first, the patient does not have any major health problems that require nursing care; second, the patient has a health problem that can be managed at home; third, the patient has a health problem that can be managed at an outpatient clinic; and fourth, the patient has a health problem that requires urgent care.
Currently, nurses providing telephone consultation usually document the reason for the phone call and the kind of nursing service they provided on paper, which is not kept as part of the formal nursing records. Thus, it is necessary to develop and computerize a triage guideline for nurses to use when they receive a phone call from a patient or family, and an electronic nursing record system for nurses to document the patient's problems and the services they provide to solve a specific problem. This system needs to be developed using standardized terminology, if the collected data are to be utilized for research and practice. In order to develop and computerize a triage guideline and an electronic nursing record system using standardized nursing terminology for telephone nursing, the content of telephone nursing consultations must be analyzed and mapped with standardized terminology. The International Classification for Nursing Practice (ICNP), a multiaxial combinatorial terminology developed by the International Council of Nurses (ICN), is used as the standardized terminology in this study [7]. The ICNP has been used for cross-mapping the nursing records of cardiology, pediatric intensive care unit, orthopedics, thoracic surgery, liver cancer, and adult intensive care unit patients [8-13] and is used for the electronic nursing record system in Korea [14-16].
With this background, we collected the health problems reported to the ophthalmological nursing station by a patient or family member after post-surgical discharge and the nursing services provided to callers, which we analyzed and mapped with ICNP ver. 1.0. The outcomes of this study can be used to develop electronic triage guidelines for a telephone nursing consultation and documentation system.
II. Methods
The narrative paper telephone nursing consultation documentations of 170 patients who underwent ophthalmological surgical procedures were analyzed. Data were collected during telephone consultations after receiving the patient's consent, from September 29 through November 30, 2008, at a tertiary teaching hospital in Seoul. These statements were analyzed using the Korean ver. of ICNP ver. 1.0 [17].
The narrative telephone nursing consultation documentations were broken down into statements. These statements were divided into three groups according to their content: 1) nursing phenomena-related statements (nursing diagnosis, patient's problem, and signs/symptoms), 2) nursing actions-related statements, and 3) other statements. This classification was validated by two ophthalmology nursing unit nurses who were familiar with ICNP: one head nurse who participated in the development of an ICNP-based electronic nursing record system, and one staff nurse with a master's degree.
Unique nursing statements were extracted by removing and combining nursing statements with the same meaning. Each unique statement was decomposed into concepts, which were then cross-mapped to the ICNP 7-axis model concepts. As a result, unique statements were classified into three groups (completely mapped, partially mapped, and not mapped) according to criteria as follows. If all concepts of the statement were mapped to ICNP concepts, this was classified as completely mapped. If any concept of each statement was not mapped to ICNP concepts, this was classified as partially mapped. If none of the concepts were mapped to ICNP concepts, this was classified as not mapped. The mapping was reviewed and validated by two ophthalmology nursing unit nurses who were familiar with the ICNP.
III. Results
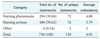
The narrative telephone nursing consultation documentations were composed of 738 statements. These statements were divided into three groups according to their content: 1) 294 nursing phenomena-related statements, 2) 440 nursing actions-related statements, and 3) 4 other statements. When the redundant statements (in terms of meaning) were removed, there were 72 unique nursing phenomena-related statements, 76 unique nursing actions-related statements, and 2 other statements, resulting in a mean of 4.92 repetitions per unique statement (Table 1).
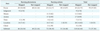
Out of 72 unique nursing phenomena-related statements, 55 statements were mapped completely to the concepts of the ICNP, 12 statements were partially mapped, and 5 statements were not mapped at all. Out of 76 unique nursing actions-related statements, 29 statements were completely mapped to concepts of the ICNP, and 47 statements were partially mapped (Table 2).
Out of the 55 unique nursing phenomena-related statements that were completely mapped to ICNP concepts, 23 statements were used to document the 'knowledge deficit' nursing diagnosis. Patients had questions regarding medicine prescribed after discharge, their next appointment to visit the outpatient department, and self-administration of medication after surgery. The remaining 32 statements were used to document physical symptoms such as 'congestion,' 'pain,' 'impaired sight,' 'dizziness,' and 'vomiting.' Examples are 'having hyperemia conjunctiva,' 'having some pain in eye,' 'having some loss of eyesight in surgical eye,' and 'having some discharge.'
Out of 29 unique nursing actions-related statements that were completely mapped to ICNP concepts, 13 statements were used to document the nursing action 'assessing.' Examples include assessing hyperemia conjunctiva, headache, side effects of medication, and loss of eyesight. The remaining 16 statements were used to document nursing actions such as 'educating,' 'explaining,' 'permitting,' 'restricting,' 'advising,' 'informing,' and 'reassuring.'
There were 12 partially mapped unique nursing phenomena-related statements due to the lack of focus concepts. Examples are 'eye feels uncomfortable,' 'no eye discomfort,' 'sudden increase in eye discomfort,' 'narrowed visual field after surgery,' 'having some floater sensation,' 'no loss of eyesight in surgical site,' 'having some double vision,' 'having some foreign body sensations,' and 'unable to open eyes because of brightness.'
Out of 47 partially mapped unique nursing actions-related statements due to the lack of focus concepts, 14 statements were statements describing the nursing action 'instructing.' Examples are instructing to observe present symptom, patient to be examined in the outpatient department, patient to apply eye drops, to lie prone, and to call hospital ward back later. The remaining statements were used to describe explaining the patient's operation name, contacting hospital insurance/hospital administration, guiding the patient's scheduled appointment to visit the outpatient department/the patient's day surgery schedule/procedure to receive a medical certificate, informing charges for the operation, giving information on discharge procedures, and giving information on admission fees.
Five nursing phenomena-related statements not mapped to the ICNP were 'shedding copious tears,' 'heard from local clinic that eye is inflamed,' 'sweat in eye,' 'unable to keep eyes open,' and 'drooping eyelids.' These five statements were direct quotes of patients' statements and were not nursing problems. They include expressions of medical diagnosis, patients' symptoms, and major concerns used to record patients' conditions.
Two unique statements that did not describe nursing phenomena or nursing actions were 'I want to contact my surgeon,' and 'I did not have any prescriptions for pain.'
From the 150 unique statements, 189 unique concepts were extracted. Among these 189 concepts, 86 (45.5%) were related to nursing phenomena and the other 103 (54.5%) to nursing actions. Of these concepts, 40 nursing phenomena concepts (21.16%) and 31 nursing actions concepts (16.4%) did not map onto the ICNP (Table 3).
'Knowledge,' 'pain,' 'congestion,' and 'sight' were frequently used concepts in describing nursing phenomena from the focus axis of the INCP. 'Low' and 'actual' were frequently used concepts from the judgment axis. 'After discharge,' 'acute', and 'postoperative' were frequently used concepts from the time axis. 'Eye,' 'laterality of surgery,' and 'conjunctiva' were frequently used concepts from the location axis (Table 4).
'Congestion,' 'pain,' and 'side effect' were frequently used concepts in describing nursing actions from the focus axis. 'Medication regime,' 'pain guideline,' and 'instruction material' were frequently used concepts from the means axis. 'Instructing,' 'assessing,' and 'educating' were frequently used concepts from the action axis. 'After discharge' and 'for about a month' were frequently used concepts from the time axis. 'Outpatient department,' 'ocular route,' and 'home' were frequently used concepts from the location axis. 'Patient' and 'family caregiver' were frequently used concepts from the client axis (Table 4).
IV. Discussion
This study was conducted to observe how a concept-based terminology can be used to describe telephone nursing consultation documentations. This study began by investigating what nurses wrote in nursing documentations through the content analysis of narrative nursing documentations. It was found that the categories of statements well reflected the telephone nursing consultation process. This in turn proved that the nursing process of assessment, intervention, and evaluation is a feasible way of structuring narrative nursing documentations.
Furthermore, the fact that 738 statements could be expressed with only 150 unique statements -- a redundancy of 4.92 times -- demonstrates the feasibility of computerizing narrative nursing documentations for electronic telephone triage.
More than 62% of 189 nursing concepts from 150 unique nursing statements cross-mapped to the ICNP. This implies that standardized terminology-based nursing statements are possible for structured data entry. Standardized terminology-based statements allow for better data collection and more ease for nurse educators and nurse researchers in reusing data for education and research.
Analysis of nursing phenomena-related statements showed that 'knowledge' was the most frequently used concept from the focus axis and 'low' was the most frequently used concept from the judgment axis. The frequent use of 'knowledge deficit' in documenting telephone nursing reflects patients' concerns about maintaining their health at home. Targets of their concern include prescribed medication after discharge and instructions after surgery.
Out of 86 concepts used to describe nursing phenomena, 40 concepts (46.5%) did not map to the ICNP. Most of the concepts not mapped to the ICNP were the focus concepts. Examples are 'discomfort,' 'narrowing visual field,' 'floater,' 'double vision,' 'foreign body sensation,' and 'photophobia,' which are frequently used in ophthalmological nursing. These concepts need to be added to ICNP ver. 1.0 in the future.
Out of 103 concepts used to describe nursing actions, 31 concepts (30.09%) did not map to the ICNP. Again, most of the concepts not mapped to the ICNP were the Focus concepts. They include concepts identified already in the analysis of nursing phenomena-related statements and other ophthalmological concepts such as 'eye drops' and '(eyeball) protection.' In addition, there are concepts-related administrative procedures such as 'scheduled appointment,' 'day surgery schedule,' 'a medical certificate,' 'operation name,' 'charges for an operation,' 'discharge procedure,' 'admission fees,' 'hospital insurance department,' and 'hospital administration.' Analysis of nursing actions-related statements showed that concepts related to nursing instruction on 'observing' such as 'instructing to observe present symptom,' on 'visiting' such as 'instructing patient visit the outpatient department/emergency department/nearby hospital,' and on 'calling' such as 'instructing to call hospital again later' are not mapped to ICNP concepts.
The mapping rate in this study was lower than that in Ryu and Park's analysis of electronic nursing records for internal medicine and cardiology patient [8]. The main reason for this difference is probably that Ryu and Park [8] cross-mapped from the electronic nursing record system to the ICNP statements that were already standardized, whereas paper-based nursing documentations were cross-mapped in this study [18].
The results of this study imply that the computerization of narrative telephone consultation documentations is feasible with a concept-based nursing terminology such as the ICNP. However, it is important to identify local terms not mapped to the ICNP and to add these terms to standardized terminology in order to improve the expressiveness of the nursing documentations [18-20].
Even though it used convenient samples of nursing consultation records documented during 9 weeks of telephone consultations in an ophthalmological nursing unit of a tertiary teaching hospital, this study provided very meaningful insights regarding telephone nursing consultations. Although this study was limited to ophthalmology nursing, our approach could also be applied to other telephone consultations in other areas of nursing. Further studies should be conducted to see how the results of this study can be used in developing a decision support system for the telephone triage and electronic telephone nursing consultation record system.


 XML Download
XML Download