

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
As the elderly population grows, the prevalence of aging-related disease and drug expenditure has increased in Korea. The population of age 65 or more has reached 9.6% of the total population in the year 2006, and is projected to be 14.3% by 2018 and 20.8% by 2026 [1]. Despite the fact that only 9.6% of the population is aged 65 or older, they still account for 25% of total health expenditure, which is a relatively high medical cost compared to other age groups [2]. An aging society implies that there is a higher prevalence of chronic degenerative disease, which leads to more prescriptions for drug therapy. About 90.9% of the elderly have chronic disease, and in Korea, it has been reported that 73.8% of the elderly have more than two chronic diseases [3]. It has also been reported that 77.7% of the elderly are currently taking at least one medication [4]. This is a common problem in many countries, for instance in the United States, where more than 80% of the elderly take more than one medication [5].
Frequent exposure to medications increases the likelihood of developing complications from drug therapy. A high rate of medication use makes older adults particularly vulnerable to medication-related problems, combined with age-related physiological changes in the way drugs are absorbed, distributed, metabolized, and excreted [6]. Inappropriate medication use in elderly patients has been linked to a large share of adverse drug reactions [7], worsening physical functions [8], and excess health care utilization. Therefore, the use of inappropriate medications by elderly patients is an important concern for patient safety and for the rational use of health care resources.
Copper [9] reported that 10-35% of the elderly report adverse effects after medication, and that 1/3 of all hospitalizations of elderly patients are partly due to adverse drug reactions. Hanlon et al. [10] reported that 35% of outpatients experience drug-related side effects; 29% of those patients revisited medical facilities, including emergency rooms, to treat these side effects.
Since the 1990s, criteria have been used to assess inappropriate medication use. At the beginning implicit criteria was developed, but which is often considered impractical to use in population-based studies. So the explicit criteria were developed by panels of experts in geriatric medicine and pharmacology. Two sets of explicit criteria, the Beers criteria [6,11,12] and Canadian criteria [13], have been used for safer drug administration and preparation, clinical education, health outcomes, and medical cost and benefits analysis for the last decade. Beers et al. [11] quantified the appropriateness of drug prescriptions for nursing home residents, and added the severity noting high or low risk in 1997 [12]. Since then, Beers criteria were updated for the Beers criteria in 2002 [6]. The Beers criteria selected inappropriate drugs for use at outpatient and long-term care facilities for the elderly by an extensive literature review and a modified Delphi method, as evaluated by twelve geriatrics and pharmacology specialists. The Beers criteria categorize the drugs into two groups, either independent of diagnosis (ID) or considering diagnosis (CD), depending on the critical condition. This method was then selected for nursing home regulation by Center for Medicare & Medicaid Service (CMS) in July 1999, and for quality indicators for managed care plans by Health Plan and Employer Data and Information Set (HEDIS) [6,14]. Zhan's classification consists of 33 categories of drugs, which are categorized as prohibited for the elderly regardless of dosage, frequency and duration; potentially inappropriate; or appropriate under certain conditions [15]. McLeod et al. [13] developed the Canadian criteria for inappropriate practices in prescribing for elderly people.
Although the Beers criteria (1997, 2003) [6,12] and the Canadian criteria (1997) [13] were developed based on an extensive literature review and expert opinions, they are applied to drugs used for patients in long-term care such as nursing homes. Thus, these criteria may not be useful to assess medications given for a short time period in an outpatient setting. In addition, it may not be possible to apply the criteria to Korean people directly, since the criteria are developed for drugs used in the United States only. Additionally, the expert consensus panel consisted of 6 different nationalities and some of the drugs in the list are not available in South Korea. Therefore, list of potentially inappropriate medication for the Korean elderly need to be developed.
The purpose of this study is to develop the list of potentially inappropriate drugs for the elderly in Korea using the Delphi technique, to reach consensus on a list from the expert panel.
II. Methods
1. Study Process
In order to identify applicable criteria for medication use for elderly persons in a community setting in Korea, this study included several steps. First, previously published criteria for potentially inappropriate drugs was reviewed and matched with the list for reimbursable drugs in Korea. Next, a survey questionnaire for the expert panel was developed. Then, opinions from the expert panel through a Delphi evaluation were compared with the Beers criteria and the Canadian criteria, and then the level of inappropriateness was determined, taking into account adverse effects and availability of substitutable drugs.
2. Selection of Drugs for Which a Decision is Required
We adopted list from Beers criteria [6,11,12], Canadian criteria [13] and Zhan's classification [15] using Fialova et al.'s therapeutic classification [16], and identified 17 therapeutic classes as potentially inappropriate drugs, regardless of the disease. While the Beers criteria [6] indicated barbiturates as a class of drugs, we specified barbiturates to include amytal sodium, pentobarbital, secobarbital, and thiopental. With regard to disease-specific potentially inappropriate drugs for the elderly, the disease code is provided from persons who are in charge of the medical records. For this category, β-adrenergic blocking agent, anticholinergics, antihistamines, antispasmodics, antidepressants, decongestants, non steroidal anti-inflammatory drugs (NSAIDs), calcium channel blocker, tricyclic antidepressants (TCA), thiazide diuretic, steroids, conventional antipsychotics, and long benzodiazepine are included.
3. Questionnaires for the Expert Panel
Adverse effects of pharmaceuticals and the drugs that can be substituted are presented in questionnaires for the Delphi evaluation. Three main questions for the expert panel members were clinical importance of side effects, availability of possible substitute drugs, and conditions for which drugs should be used. The first two questions were answered on 4-response Likert scales and the last question was open ended.
The drug-related side effects were summarized after a review of Beers et al. [11,12,6], McLeod et al. [13], and Zhan et al. [15], and substitutable drugs were as specified by the WHO Collaborating Center [17], KIMS data, and MICROMEDEX Healthcare Series (Figure 1). The second round questionnaires were consisted of evaluating appropriateness of indicators using potentially inappropriate drugs for the elderly and suggesting other opinion in the second round if they did not agree with results from the first round.
4. The Expert Panel Members and Data Collection
The expert panel consisted of 14 geriatric specialists, including 7 family medicine specialists, 3 psychiatrists, 1 neurologist and 3 clinical pharmacists. The expert panel performed the survey in two rounds.
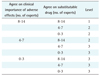
From the first round of Delphi evaluations, the drugs were categorized into three groups based on answers from the first two questions. Drugs for which more than 50% of panel members answered level 3 or 4 for both questions were classified as group 1. If less than 50% of panel members answered level 3 or 4 for either question, those drugs were identified as group 2 and the remaining drugs were identified as group 3 (Table 1).
In the second round, the expert panel could suggest their opinion if they did not agree with results from the first round and the utility data of drugs with group 1 were provided for reference. The categories were adjusted and finalized into three groups for the elderly: drugs that should be avoided (group 1), those that need to be monitored (group 2), and drugs with a low level of risk (group 3).
III. Results
1. Potentially Inappropriate Drugs, Independent of Diagnosis
The expert panel developed a list of 57 potentially inappropriate ingredients for the elderly, independent of diagnosis, among the 60 ingredients. Forty-two drugs were classified into group 1 (drugs that need to be avoided), 13 drugs into group 2 (drugs that need to be monitored), and 2 drugs into group 3 (drugs with minimal harm to the elderly) (Table 2).
Table 2 shows the list of potentially inappropriate drugs, independent of diagnosis. Among all of the drugs from drugs of both Beer Criteria [6] and Canadian Criteria [13], thirty drugs were not listed and three ingredients that are considered to be inappropriate for the elderly were excluded. The drugs that were excluded were antibacterial (nitrofurantoin), antiemetic (trimethobenzamide) and vasodilatory (cyclandelate). The unlisted drugs were analgesic/anti-inflammatory (mefenamic acid, phenylbutazone), anticholinergic (tripelennamine, dexchlorpheniramie, clidinum, clidinum-chlordiazepoxide), antidiarrheal (diphenoxylate), antiemetic (trimethobenzamide), antihypertensive (guanadrel, guanethidine), antipsychotic (perphenazine-amitriptyline), diuretic (ethacrynic acid), hormonal (dessicated thyroid), laxative (mineral oil), niacin, sedative (meprobamate, quazepam, halazepam, chlorazepam), stimulants (amphetamine and anorexics, methylphenidate) and vasodilatory (isoxsuprine, nylidin).
Iron supplements were categorized into group 3. For the treatment of anemia, a daily dose of less than 325 mg per day is recommended, due to the risk of constipation. NSAIDs with a high risk of central nervous system side effects, gastrointestinal ulcer bleeding, renal failure, high blood pressure and heart failure are included in group 1. Acetaminophen, for minor pain relief, or other NSAIDs, with fewer side effects, are recommended for a minimum period as substitute drugs. For chronic pain, such as arthritis, COX-2 inhibitors are recommended for patients that do not have any risks for cardiovascular events, such as myocardial infarction. Narcotic analgesics, meperidine and pentazocin are categorized into the group 1, and are also included in the Beers, Canadian, and Zhan criteria. Due to adverse side effects of these analgesics, including confusion and hallucination, the risk that these may occur among patients with delirium or dementia would have increased. For severe pain relief, other narcotic analgesics such as codeine, morphine or hydromorphine are recommended. Aspirin and clopidogrel are relatively safe anticoagulants to use for the elderly. Ticlopidine is categorized into group 1, due to its side effect on inducing myelosuppression. Anticholinergic drugs are categorized into group 1, due to the adverse effects of confusion, hallucination, worsening dementia, sedation, dry mouth, urinary retention, hydrodipsomania and ischuria. Second-generation antihistamine drugs are recommended for use instead of antihistamine/anticholinergic combination drugs. Among antispasmodic agents, dicyclomine and propantheline are categorized into group 1. It is recommended to discontinue use of anticholinergic agent medications unless severe gastrodynia is present. Oxybutynin, which is rapidly absorbed, is recommended to use for only a short period. Antidepressants with strong anticholinergic effects, such as amitriptyline, imipramine and doxepin, are categorized into group 1. For substitute drugs, TCAs without persistent active metabolites, such as nortryptyline, desipramine and protriptyline or selective serotonin reuptake inhibitor (SSRI), or with a short half-life such as fluvoxamine, are recommended. Fluoxetine, which has a long half-life, is categorized into group 1. Muscle relaxant or antispasmodic agents, such as carisoprodol, chlorzoxazone, cyclobenzaprine, metaxalone, methocarbamol and orphenadrine, also have strong anticholinergic side effects. Therefore, instead of these, non-pharmacological therapy, medical nutrition therapy or physical therapy is recommended. Antihypertensive drugs with central nervous system side effects, such as clonidine, methyldopa and reserpine, are categorized into group 1 or 2. These medications are rarely used; however, they are required to be taken into consideration. An alpha blocker such as doxazocin, and a short-acting calcium blocker such as nifedipine, are in high risk that they carry a high risk of patient fall due to orthostatic hypotension. Instead, a long-acting calcium blocker and a low dose of diuretics are recommended for hypertensive drugs. Benzodiazepines are less addictive and have fewer side effects than barbiturates (group 1), including fewer falls, fractures and CNS side effects (e.g., stupor). However, diazepam, chlordiazepoxide and flurazepam with a long half-life are categorized into group 1, due to a high risk of side effects with an increased effect of sedation. Instead, benzodiazepines (group 2) with a short half-life are recommended. The increased sensitivity of drug effects among the elderly requires lower doses; lorazepam 3 mg/day, oxazepam 60 mg/day, alprazolam 2 mg/day, and temazepam 15 mg/day, as needed for a minimum period.
2. Potentially Inappropriate Medical Use in Older Adults Considering Diagnoses or Conditions
As shown in Table 3, there were 93 drugs potentially inappropriate for the elderly with 29 diagnoses, group 1, group 2, and group 3 included 63, 28, and 3 drugs, respectively. Drugs for anorexia and malnutrition (dextroamphetamine, methamphetamine, pemolin) and cognitive impairment (dextroamphetamine, methamphetamine, and pemollin) were excluded from Beers's criteria [6] because they were not included in the reimbursable drug list in Korea. Chlordiazepoxide-amitriptyline, clidinium-chlordiazepoxide, quazepam and halazepam needed to be carefully monitored for chronic obstructive pulmonary disease (COPD) patients, and guaethidine for patients with depression were excluded because they are not on the market in Korea. Phenylpropanolamine hydrochloride for hypertension was also removed from the US market in 2001 and Beers criteria. On the other hand, anorexia and malnutrition (fluoxetin) was removed based upon the consensus among the researcher.
Among 29 diseases, the clinical importance of syndrome of inappropriate secretion of antidiuretic hormone (SIADH)/hyponatremia has not been appreciated. Therefore, Citalopram and fluoxepine are categorized into group 3. Because TCAs in group 1, including amitryptyline, doxepin, imipramine, carry a high risk of arrhythmia due to an increase in electrocardiogram (ECG) QT interval, SSRIs are recommended as antidepressants for elderly patients with arrhythmia. Anticholinergic drugs, such as oxybutynin and tolerodine (which have side effects such as urinary retention) antihistamine agents, antispasmodic agents, antidepressants, and muscle relaxants are categorized into group 1. Any adverse effects of anticholinergic drugs, muscle relaxants and barbiturates on the CNS should be carefully monitored. It is recommended to stop the use of methylphenidate (group 1). With an increase in the prevalence of COPD among the elderly, long acting drugs such as diazepam, chlordiazepate and chlordiazepoxide with a risk of respiratory inhibition are categorized into group 1. Group 1 included the substitute drug, propanolol (group 1), which inhibits bronchodilatation. For patients with hypertension, drugs that interact with the sympathetic nervous system, such as amphetamines, phenylpropanolamine (approval cancelled), pseudoephedrine and appetite suppressants, are categorized into group 1. For insomnia patients, drugs with stimulatory effects, such as amphetamines, methylphenidate, monoamine oxidase inhibitor (MAOI), and theophylline are included in group 1. Since antidopaminergic and anticholinergic agents could worsen Parkinson's disease, it is recommended that metoclopramide, gastroprokinetic agents. And tacrine, an anticholinergic agent, be substituted for domperidone and other Alzheimer medications, respectively. Trycyclic antidepressants with a risk of orthostatic hypotension and syncope are categorized into group 1. For patients with stress-induced urinary incontinence, alpha-blockers including doxazocin, prazocin and terazocin and TCAs are categorized into group 1, due to worsening urinary incontinence.
IV. Discussion
As the aged population grows, the prevalence of chronic degenerative diseases has increased, along with the number of prescriptions and drug interactions from polypharmacy for elderly patients. In other countries, along with the United States of America, the criteria for potentially inappropriate drugs for elder patients, such as the Beers criteria [6,12] and the Canadian criteria [13], have already been proposed for use, based on assumption that patients at nursing home will use them for long-term.
Assuming the current growth rate of aged people, it is projected to be an aged society by 2018 and a post-aged society by 2026. Therefore, it is very important to reconsider the quality and effectiveness of pharmaceutical therapy for the elderly. For the elderly with frequently prescribed drugs, it is crucial to prevent side effects and to improve safety by minimizing inappropriate drug use. Health Insurance Review & Assessment Service (HIRA) already has been performing quality assessment for medical services since 2001, to guarantee the delivery of safe and effective medical services. It has been suggested that criteria of drug prescription safety for the elderly should be developed for patient safety issues [18].
In this study, the list for inappropriate drugs for elderly was determined by using the Delphi evaluation from the expert panel, consisting of 7 geriatric specialists, 3 geriatric psychiatrists, a neurologist and 3 clinical pharmacists. The level of inappropriateness was determined by taking into account the clinical significance of any adverse effects of the drugs and the availability of substitute drugs: group 1 lists drugs that need to be avoided, group 2 lists drugs that need to be monitored, and group 3 lists drugs that have minimal danger to the elderly, and thus do not need to be monitored.
The expert panel developed a list of 57 potentially inappropriate ingredients for the elderly, ID among the 60 ingredients. Forty-two drugs were classified into group 1, 13 drugs into group 2, and 2 drugs into group 3. Ninty-three drugs were potentially inappropriate for the elderly with 29 diagnoses, group 1, 2, and 3 included 63, 28, and 3 drugs, respectively.
The list should be considered for application in practice as follows. First, the list of potentially inappropriate drugs was developed with some modification, but complements the Beers criteria is focused on a narrow scope of treatment, which resulted in the agreement on the adverse effects of the drugs in the elderly. However, it is not possible to evaluate whether prescription of these drugs is valid for a wider scope of treatment [19,20]. In addition, the use of inappropriate drugs, which is based on Drug Use Review (DUR) criteria, would be more applicable for an outpatient setting, in terms of drug-to-drug and drug-to-disease interactions. Studies have shown that the Beers criteria fit better for an inpatient setting [21,22]. In addition, it has been criticized that there are no criteria available to identify false, abusive and overlapping prescribing practices, which need to be monitored in separate ways.
Second, it may not be proper to use substitute drugs for potentially inappropriate drugs. For example, TCAs have been on the market for long enough to guarantee their safety in some specific situations. For instance, amitriptyline is often prescribed for diabetic neuropathy and has been shown to be more effective and inexpensive than other drugs [23]. For example, TCAs have been widely used for a long time, the safety would be guaranteed. Furthermore, substituted drugs will be safer and inexpensive.
Third, it is difficult to apply monitoring potentially inappropriate medication use CD. The patients that have been identified to have a disease using the claims data with the corresponding disease code might be lower than what is actually prevalent. For instance, in order to select a patient with asthma, hypertension, and depression, more than one claim with the disease code and prescribed drugs must be used [24].
Finally, it is important to keep in mind that the criteria for potentially inappropriate drugs for the elderly are only a screening tool. In special cases, it would not be proper to apply these criteria. For example, it would be appropriate to take amitriptyline when the patient needs strong anticholinergic drugs to treat a major depressive disorder and Parkinsonism [11]. Hence, for an effective use of criteria, the severity and symptoms of the disease should be accompanied in administrative data. In other words, the administration of drugs should be approved with supplementary patient information for unavoidable circumstances. In addition, research on the outcome of adverse effect for potentially inappropriate drug administration for elder patients must be performed.
This study especially aimed to develop the list of potentially inappropriate drugs for elderly patients using the Delphi evaluation from the expert panel, consisting of seven geriatric specialists, three geriatric psychiatrists, a neurologist and three clinical pharmacists. This list was extracted from Beers criteria, Zahn's classification, and Canadian criteria. Beers criteria, developed by literature review and 12 panelists' consensus using modified Delphi method, identified 48 individual medications or classes of medication to avoid in older adults and their potential concerns and 20 disease/conditions and medication to be avoided in older adults with these conditions. Zhan's classification was restricted to a subset of 33 drugs from the Beers criteria because Medical Expenditure Survey (MEPS) does not include sufficient detail on drug dosage, frequency, and duration of administration. Canadian criteria was developed by 32-member national panel's consensus and was consisted of list of 71 practices in prescribing for elderly people.
It is expected that the list of inappropriate prescribing for the elderly people would be regularly checked if it is to be helpful to physicians. For existing criteria based on literature review and many drugs prescribed for elderly people, there is a dearth of evidence-based guidelines, so we relied on a consensus panel without own literature review. We did not perform surveys on medical record to search for acute admission due to adverse drug event because this list will be applied to pattern analysis using administrative data.
Despite these limitations, the Beer criteria have been widely utilized for screening in community settings. Willcox et al. [25] and Zhan et al. [15] used NMES or MEPS data to investigate the prescription rate of inappropriate drugs for the elderly. Allard et al. [26] investigated the prescription rate of inappropriate drugs by the physicians practicing in Sherbrooke, Quebec, Canada. Fillenbaum et al. [22] and Blalock et al. [27] also investigated the prescription rate among the elderly in community settings.
In conclusion, the criteria can be used to improve the quality of pharmaceutical therapy and the list of potentially inappropriate drugs should be used with caution. Further efforts are needed to revise periodically a list of inappropriate drugs for the elderly reflecting the concurrent medical care. Our study focuses on developing list of inappropriate medication for the elderly patients. Further studies are needed to assess the problems of inappropriate drugs in elderly patients and understand factors affecting use of the inappropropriate drugs. Moreover, further challenges to assess hospitalization due to potentially inappropriate drugs-related adverse event are remained.














 XML Download
XML Download