

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Previous studies have shown that inflammation plays an important role in the initiation and progression of cardiovascular disease (CVD).1)2) Given the association of inflammation with type 2 diabetes mellitus (T2DM),3)4) the role of inflammation may be additive for the development of atherosclerosis in T2DM patients. Currently, the neutrophil-to-lymphocyte ratio (NLR), a simple and inexpensive method for assessing inflammatory status, has been investigated as a new predictor for cardiovascular risk.5)6) However, few studies have investigated the combined impact of T2DM and inflammatory markers including NLR on coronary artery disease (CAD) or carotid artery atherosclerosis. Because NLR was also found to be independently associated with the coronary calcium score,7) we hypothesized that there exists an association between NLR and the severity of CAD. The objective of this study was to evaluate the combined impact of T2DM and NLR on significant CAD and carotid artery atherosclerosis assessed by carotid artery ultrasound (US).
Methods
Study population
A total of 828 patients admitted to our institution for suspected CAD, who underwent carotid artery US and coronary angiography from January 2013 to October 2014, were enrolled in this study. All patients were evaluated for the presence of cardiovascular risk factors such as hypertension, hyperlipidemia, T2DM, stroke history, obesity, and smoking status. Height and weight were measured, and body mass index (BMI, kg/m2) was calculated. Patients were considered hypertensive if they were previously diagnosed with hypertension, used any anti-hypertensive medications, or had a systolic blood pressure ≥ 140 mm Hg and/or a diastolic blood pressure ≥ 90 mm Hg. T2DM was defined as a fasting plasma glucose level of more than 126 mg/dL on two consecutive readings, a previous diagnosis of T2DM or the use of anti-diabetic medications such as oral anti-diabetic agents or insulin. Patients were asked whether they were current smokers or nonsmokers. The presence of dyslipidemia was assumed if participants were taking lipid-lowering drugs or had a high cholesterol level. Obesity was defined as a BMI above 25 kg/m2, as per the Korean Society for the Study of Obesity.8) Significant CAD was defined as the presence of at least one vessel with stenosis > 50%, and significant carotid atherosclerosis was defined as an increased intima media thickness (IMT) ≥ 0.9 mm or the presence of a plaque. Acute coronary syndrome (ACS) was assumed if participants were diagnosed with myocardial infarction or unstable angina. Patients being treated for systemic diseases affecting white blood cell counts, such as hematopoietic disorders, and those with a history of malignancies and/or treatment with chemotherapy, evidence of any concomitant inflammatory disease, acute infection, chronic inflammatory status, history of glucocorticoid therapy within the past 3 months, and secondary hypertension were excluded from the study. This study was approved by the Institutional Review Board of Kosin University School of Medicine, and all patients provided written informed consent before participation.
Laboratory parameters
Complete blood count, which included total white blood cells, neutrophils, lymphocytes, and platelets, was obtained at the time of admission. Inflammatory markers including NLR and high sensitivity C-reactive protein (hs-CRP) were measured. NLR was calculated as the ratio of the absolute neutrophil count to the absolute lymphocyte count. Both of these values were obtained from the same automated blood sample.
Carotid artery ultrasound
Participants rested for at least 10 minutes in the supine position prior to carotid US examination. We scanned the bilateral common carotid arteries (CCA), carotid bifurcations and the origins of the internal carotid arteries in longitudinal and transverse planes using a 14-MHz transducer (Philips iE33, Philips Medical Systems, Bothell, WA, USA). A single observer, blinded to participant demographic data and cardiovascular risk profile, measured the combined thickness of the intima and media of both CCAs. After designating a region of interest in the far wall of the CCA, the mean IMT was estimated in a region free of atherosclerotic plaques using an automatic tracking system. 9) An increased IMT was defined as ≥ 0.9 mm in one or both carotid arteries, and the presence of atherosclerotic plaque was defined as a focal structure that encroached into the arterial lumen by at least 0.5 mm or 50% of the surrounding IMT value or demonstrated a thickness of > 1.5 mm as measured from the media–adventitial interface to the intima–lumen interface.10)11) The plaque area was measured by tracing the plaque border, and the total plaque area (TPA) was the sum of all plaque areas between the clavicle and the angle of the jaw.12) In addition, carotid wall shear stress (WSS) was calculated using the Poiseuillian parabolic model of velocity distribution according to Gnasso et al.13) Carotid artery atherosclerosis was defined if there was increased IMT or the presence of plaque.
Coronary angiogram
An INTEGRIS BV 5000 (Philips Medical System, Best, the Netherlands) was utilized to visualize the coronary artery stenosis. Quantitative measurements were analyzed using a workstation with dedicated software (WIN 32 version 3.3). Patients with at least one lesion of > 50% stenosis within the main branches of the coronary arteries were considered to have significant CAD. Patients with minimal atherosclerotic lesions (≤ 50% stenosis) in the coronary arteries were not included.
Statistical analysis
The differences in baseline characteristics between patient groups (not-significant CAD and significant CAD) were tested using the t-statistics for continuous variables and using the chi-square statistics (or the Fisher exact test) for categorical variables. Logistic regression models were employed to investigate the association between significant CAD and baseline clinical and laboratory covariates including NLR and T2DM. Avoiding multi-collinearity, we performed a variable selection in stepwise fashion. The calibration and discriminability of logistic regression models were validated by the Hosmer-Lemeshow test and C-index, respectively. Utilizing likelihood ratio tests and the Delong's tests,14) we compared the goodness-of-fit and discriminability of four different logistic regression models: Model 1 includes conventional cardiovascular risk factors such as age, gender, smoking status, high density lipoprotein (HDL) cholesterol, hemoglobin; Model 2 extends Model 1 with T2DM; Model 3 extends Model 1 with NLR; Model 4 extends Model 1 with T2DM and NLR, respectively. After verifying the prognostic value of NLR on a continuous scale, we also investigated the clinical relevance of the categorized NLR that classifies patients into three risk groups (low, intermediate, high). The cut-values for the NLR risk groups were carefully searched to minimize information loss in terms of loglikelihood differences discretizing the continuous variable of NLR.15) One-way analysis of variance or homogeneity tests using the chi-square statistics were performed to compare the NLR risk groups (low and high) further classified by T2DM status. In hypothesis testing, a significance level of 0.05 was chosen. All statistical analyses were performed using R (http://www.r-project.org).
Results
Patient characteristics
The baseline clinical and laboratory characteristics of the study groups (not-significant CAD and significant CAD) were summarized in Table 1. Patients with significant CAD were order and more likely to be male; they more frequently had a smoking habit, hypertension and T2DM (p < 0.001); they had higher levels of hemoglobin, cholesterol profiles, and NLR (p < 0.001). Also, there was a positive correlation between NLR and the severity of CAD (Fig. 1).
Prognostic value of NLR and T2DM with significant CAD
According to simply logistic regression analysis, the marginally significant baseline clinical and laboratory covariates including age, gender, smoking status, hypertension, total cholesterol, HDL cholesterol, low density lipoprotein cholesterol, hemoglobin, T2DM, and NLR were entered into a multivariable logistic regression model (Table 2). According to the final model selected in stepwise fashion, both NLR [adjusted odds ratio (OR), 1.25; 95% confidence interval (CI), 1.13–1.4; p < 0.001] and T2DM (adjusted OR, 1.72; 95% CI, 1.17–2.52; p = 0.006) were independent prognostic factors significantly associated with significant CAD after adjusting age, gender, smoking status, HDL cholesterol and hemoglobin (Table 2). There was no evidence against the goodnees-of-fit of the fitted model (Hosmer-Lemeshow test statistic χ2 = 10.71; df = 8; p = 0.2188).
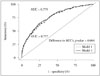
As seen from Table 3, the incremental effect of NLR and T2DM on significant CAD was investigated by comparing four different logistic regression models. According to the comparison among these models, NLR together with T2DM significantly improves the goodnees-of-fit and discriminability of the Model 1 (loglikelihood difference, 15.72; p < 0.001; C-index difference, 2.28; p = 0.004) (Fig. 2).
Optimized cut-values of NLR
The upper and lower cut-off values of NLR determined objectively by minimizing the information loss in categorizing NLR were estimated to be 1 and 2, respectively. Among a total of 828 patients, 53 (6.4%), 424 (51.2%), and 351 (42.4%) patients were assigned into three risk groups as follow: the low risk group if NLR ≤ 1, the intermediate risk group if 1 < NLR ≤ 2, and the high risk group if NLR > 2. As shown in Table 4, the categorized NLR was also a significant independent prognostic factor. Compared with the low risk group, the adjusted OR of the intermediate risk group and the high risk group were estimated to be 6.40 (95% CI, 2.07–29.50; p = 0.005) and 11.83 (95% CI, 3.81–54.51; p < 0.001), respectively.
Relation of subgroups (by NLR level or T2DM status) with clinical variables
Patients were classified into four subgroups by NLR risk groups (low or high) and T2DM status (non-T2DM or T2DM). The relations of theses subgroups with several clinical variables are presented in Table 5. T2DM patients belonging to the high NLR risk group (NLR > 2) had the greatest prevalence of significant CAD and carotid artery atherosclerosis; they also showed the largest TPA (non-T2DM with low NLR; 0.09 ± 0.21 vs. non-T2DM with high NLR; 0.20 ± 0.42 vs. T2DM with low NLR; 0.01 ± 0.04 vs. T2DM with high NLR; 0.40 ± 0.70 cm2, p < 0.001) and the lowest mean WSS (non-T2DM with low NLR; 2.58 ± 0.85 vs. non-T2DM with high NLR; 2.47 ± 0.81 vs. T2DM with low NLR; 2.68 ± 0.80 vs. T2DM with high NLR; 2.28 ± 0.83 dyne/cm2, p < 0.001); they most frequently had three-vessel disease and underwent percutaneous coronary intervention and ACS.
Discussion
In the present study, we found that both NLR and T2DM were independent prognostic factors significantly associated with significant CAD and that NLR and T2DM added significant incremental value compared with that furnished by conventional cardiovascular risk factors including age, gender, smoking status, HDL cholesterol, hemoglobin. Also, T2DM patients with high NLR had the greatest prevalence of significant CAD and carotid artery atherosclerosis. Our results suggest an additive impact possibly contributed by T2DM together with high inflammatory state on the development of systemic atherosclerosis.
Previous studies have shown that inflammation plays an important role in the initiation and progression of various chronic diseases16) including CVD.3)9) T2DM is frequently associated with inflammatory status17) and there was a positive association between low-grade inflammation and diabetes even in a population-based sample without any evidence of CVD. Insulin resistance is increasingly acknowledged as an independent risk factor for CVD,4) and several studies suggested the relationship between systemic inflammation and insulin resistance, which may play a decisive role in the pathogenesis of T2DM.18)19)20) Among various inflammatory markers, white blood cell count and its subtypes are associated with increased cardiovascular risk factors.5)6) Recently, NLR has emerged as an important inflammatory marker, and a high NLR is reported to be associated with a wide spectrum of CVD, including non-dipping blood pressure patterns,21) CAD,8) atrial fibrillation,6) chronic kidney disease including predialysis and dialysis patients22) and ACS.23) Previously, we showed that NLR > 2.6 was useful in predicting the long-term adverse events in patients who have undergone percutaneous coronary intervention with a drug-eluting stent.24) Although there is limited data on the association between NLR and T2DM, a high NLR value was reported to be a reliable predictive marker of insulin resistance.4) Recent study showed that NLR is increased among diabetic patients and is independently associated with the prevalence and severity of CAD in the same population.25) Similarly, our results showed that T2DM patients had higher NLR values and high NLR values were associated with the higher prevalence of significant and/or severe CAD and carotid artery atherosclerosis in patients with T2DM, which suggest a synergistic link between T2DM and inflammation. Moreover, the combined presence of T2DM with a high NLR was the strongest predictor of CAD, implicating a possible synergistic impact of T2DM and inflammation on coronary atherosclerosis. In this study, because we included the patients with ACS which might increase the white blood cell counts and NLR, we performed sensitivity analysis separately for the patients without ACS (n = 733) as the univariate/multivariate analysis. From the results for the patients without ACS were consistent with those for the total population, we may confirm that the relationship NLR and the presence of significant CAD can apply to the patients without ACS.
The other unique finding of our study was the association between T2DM, NLR and various variables of carotid artery atherosclerosis. Typically, carotid IMT is considered to be an early index of atherosclerosis. It has been related to cardiovascular risk factors as well as the severity of coronary atherosclerosis, and it can be used to predict cardiovascular events.26)27) Recently, carotid plaques, which reflect a more advanced stage of atherosclerosis, have been shown to be more closely related to CAD and to predict coronary events with more accuracy than IMT.28) Additionally, carotid WSS is an important determinant of endothelial cell function, and there is increasing evidence that low WSS induces expression of an atherogenic endothelial gene profile.29) In our study, we observed that T2DM patients with a high NLR had the highest carotid IMT and TPA and the lowest mean WSS when compared to other groups. This suggests that NLR might play a role in the severity of carotid atherosclerosis.
Traditionally, hs-CRP is measured because it is a well-known and well-established inflammatory marker. However, NLR can easily be calculated using routine clinical tests, so it is more cost-effective than measuring an additional inflammatory marker. Moreover, low lymphocyte counts may reflect poor general health and physiologic stress via redistribution of lymphocytes to lymphatic organs and lymphocyte apoptosis.30) Thus, the NLR can give us information not only about systemic inflammation via high neutrophil counts, but also about patient stress responses via low lymphocyte counts. Moreover, because neutrophils are activated in ACS and have been shown to infiltrate atherosclerotic lesions, they play a key role in destabilizing of atherosclerotic plaques.31) In our study, NLR, but not hs-CRP, was a predictive risk marker for the significant CAD and significant carotid atherosclerosis. We cannot account for the precise mechanism, but considering the characteristics of our study group comprised with relatively young patients and stable angina, 32)33) our findings might support the role of NLR as a simple, inexpensive and readily available marker and index of atherosclerosis.
This study had several limitations. First, this was an observational and single-institution study. Second, assessment of CAD was limited to visual interpretation of only major coronary arterial lesions. Third, the cut-off values of NLR found in this study were objectively determined based on our study population that may be heterogeneous compared to one in the previous studies. The possibility of the existence of universal time-invariant cut-off values, regardless of diverse patient ethnic backgrounds, study designs, statistical methods, and so on, certainly need validation by multi-center and multi-county independent studies in the future. Fourth, adequate control of blood glucose levels is an important factor in the coronary outcomes of diabetic patients; however, our data were not classified by hemoglobin A1c or fasting blood glucose because of missing data. Finally, with no follow-up data, we were limited in our ability to predict long-term outcomes. Therefore, a larger, prospective, randomized study is required to confirm our findings.
In conclusion, NLR is increased in patients with significant CAD, and a high NLR or the presence of T2DM is an independent, synergistic, predictive risk factor associated with the prevalence and severity of CAD. Our study implies that patients with T2DM together with high inflammatory state would be more vulnerable to significant coronary or carotid atherosclerosis, which might lead to a poor cardiovascular outcome. Further studies are now needed to confirm the present results and to evaluate underlying pathophysiological mechanisms.






 XML Download
XML Download