

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
At present, acute appendicitis is one of the most common surgical conditions, requiring an emergency operation and accounting for 4% to 8% of all emergency department (ED) visits [1]. Situs inversus totalis (SIT) is rare congenital disease in which the thoracic and abdominal organs are transposed [2-5].
The most common symptom of acute appendicitis is right lower abdominal pain. Therefore, in patients with left lower-quadrant pain, we do not include acute appendicitis in the typical differential diagnosis. However, in patients with SIT, left lower-quadrant pain can be a symptom of appendicitis, and misdiagnosis or perforation of the appendix may occur. We report an unusual case of left-sided appendicitis with SIT.
CASE REPORT
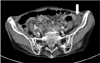
An 86-year-old woman arrived at the ED with abdominal pain. The pain started 6 hours before she arrived at the ED and was localized to the periumbilical area. The patient also complained of nausea, without vomiting or diarrhea. The patient was on hypertensive medications for 10 years with no past history of diabetes mellitus or hepatitis. Physical examination revealed a soft and flat abdomen with left lower-quadrant tenderness without rebound tenderness. Her initial vital signs were as follows: blood pressure, 152/62 mmHg; heart rate, 68/min; respiratory rate, 18/min; and body temperature, 37.1℃. The plain chest X-ray revealed the presence of dextrocardia (Fig. 1). Laboratory results revealed a normal white blood cell count (9,900 × 109/L) with neutrophils accounting for 83% of the cell population. Other laboratory results, including blood chemistry and urinalysis, were within the normal range. Abdominal computed tomography (CT) revealed the presence of a contrast-enhanced dilated appendix (maximal diameter 1.1 cm) and fatty streaks with transposed intra-abdominal organs (Figs. 2, 3). Under the impression of acute left-sided appendicitis, a laparoscopic appendectomy was conducted on the day the patient visited the ED. An 11 mm umbilical port was placed with open technique with telescope. The second 5 mm trocar with working port was introduced in the left side of the abdomen at the level of umbilicus and the third 5 mm trocar was placed in the suprapubic region (Fig. 4). The operative findings showed an inflamed, non-perforated vermiform appendix with minimal fluid collection around the Douglas pouch (Fig. 5). The mesoappendix was ligated with open type endoloop and the base was ligated with endoloop. The operative time was 28 minutes. Pathology confirmed the presence of acute suppurative appendicitis. The patient was discharged on the 4th postoperative day without any complications.
DISCUSSION
Situs inversus (SI) is a congenital positional anomaly in which the abdominal viscera develops in the wrong position. The condition is known as SIT when both the thoracic and abdominal organs are transposed. SI is an autosomal recessive congenital defect, and the incidence in the general population is only 0.001 to 0.01% [2,3].
Acute appendicitis is one of the most common causes of acute abdominal pain and requires an emergency surgical operation [1]. The typical symptoms of appendicitis begin with vague abdominal discomfort around the epigastric or periumbilical region. Several hours later, the pain migrates to the right lower quadrant.
In the general population, left lower-quadrant pain can be caused by many diseases. As for gastrointestinal causes, there are acute sigmoid diverticulitis, intestinal obstruction or perforation, incarcerated hernia, enteritis, and atypical right-sided appendicitis and left-sided appendicitis. As genitourinary causes, there are renal colic, cystitis, epididymitis, prostatitis, testicular torsion cyst and other causes including left ovarian disease, pelvic inflammatory disease, and mesenteric ischemia [1,5,6]. Primarily, there are two different anatomic anomalies attributed to a left-sided appendix: SI and malrotation of the midgut loop. In normal development, the midgut rotates in a 270-degree counterclockwise direction and the position of the appendix lies in the right lower quadrant of the abdomen. SI develops when the rotation is made in a 270-degree clockwise direction and results in complete reversal of all abdominal viscera and a left-sided appendix. Malrotation develops when there is nonrotation or incomplete rotation of the midgut loop around the axis of the superior mesenteric artery [6]. Because of the unusual displacement of the abdominal viscera in SI, the symptom of acute appendicitis can involve left lower-quadrant pain, making diagnosis very difficult in these patients. Concerning the pain location of left-sided appendicitis, Akbulut et al. [4] reported that 62% of the patients presented with left lower quadrant pain, 14% with right lower quadrant pain, and 7% with bilateral pain. Because the nervous system may not show corresponding transposition, pain location may be confusing, so preoperative diagnosis has been made in only 51% of the patients [4].
The diagnosis of SIT can be based on chest X-ray, ultrasonography, and CT images [4,5]. Plain films are not helpful in the diagnosis of appendicitis but important in the diagnosis of SIT. Sonography is a widely used modality in the diagnosis of appendicitis but it is operator-dependent and has difficulty in patients with large body habitus or with overlying bowel gas [4]. CT is especially helpful in the detection of appendicitis with SIT or malrotation [6]. In our case, a chest X-ray revealed the existence of dextrocardia, which suggested SIT. The patient also complained of left lower-quadrant pain. We therefore suspected left-sided appendicitis with SIT and conducted abdominal CT to establish the diagnosis. An emergency laparoscopic appendectomy was then performed.
Laparoscopic appendectomy in SIT was reported first by Contini et al. [7] in 1997, but the technical procedure was not described. In regard to port site, Palanivelu et al. [8] used a 10 mm suprapubic port as right working port and a 5 mm umbilical port as camera port in the left-sided appendicitis, but there were no standard port positions and they adopted a tailored approach to modify the port placements according to the basic principles of laparoscopy triangulation and ergonomy. Golash [9] used a 10 mm port in the left iliac fossa as a working port and a 5 mm port in the suprapubic region.
Appendix pedicle was ligated intracorporeally but appendectomy was conducted extracorporeally. We used a 5 mm trocar in the left-side abdomen as a working port and operated it with the left hand, and a 5 mm suprapubic trocar as a supplementary port. These trocar placements were mirror image placements of the surgical instruments for right-sided appendectomy, so a right-handed operator used their left hand as the dominant. As a result, the operative time was 28 minutes; slightly longer than that of routine right-sided appendectomy. Oms and Badia [10] reported that handedness could influence the performance of operation of SI and we speculate that a left-handed operator could overcome this handicap more conveniently. We used endoloop for the ligation of the mesoappendix. This procedure was difficult with the left hand so we recommend the use of ultrasonic scissors or bovie coagulation instead of endoloop for the ligation of the mesoappendix. Laparoscopy is considerably beneficial both in terms of the differential diagnosis and as a definitive surgery in appendicitis in SI patients because the diagnosis is difficult and the location of the appendix varies [8,9].
In conclusion, in patients with left lower-quadrant pain, if the chest X-ray shows dextrocardia, we should suspect left-sided appendicitis. A strong suspicion of appendicitis and an emergency laparoscopic operation after confirmation of the diagnosis by imaging modalities including abdominal CT or sonography can reduce the likelihood of misdiagnosis and complications including perforation and abscess. Laparoscopic appendectomy in SI was technically more challenging because of the mirror nature of the anatomy.




 XML Download
XML Download