

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Hepatic resection and liver transplantation are considered a curative treatment for hepatocellular carcinoma (HCC) within the Milan criteria. In this study, we examine the outcome of hepatic resection for HCC within the Milan criteria, and determine the effectiveness of hepatic resection as the primary treatment for HCC within the Milan criteria in Child-Pugh class A.
Methods
110 patients underwent curative surgical resection for HCC in Child-Pugh class A between August 1991 and June 2008. Fifty-six patients met Milan criteria (Group M) and the remaining 54 did not (Group N).
Results
Overall survival rates at 1, 3, and 5 years were 92.6%, 72.5% and 54.6% versus 70.4%, 43.1%, and 28.7% in Group M and Group N, respectively (P=0.0043). The corresponding disease-free survival rates were 81.5%, 69.7%, and 38.2% versus 46.0%, 32.9%, and 26.9% in Group M and Group N (P=0.0012). HCC recurred in 25 patients in Group M (44.6%) and 35 patients in Group N (64.8%)(P=0.034). Outcomes of hepatic resection in Group M were significantly better compared to Group N.
Figures and Tables
Fig. 1
Comparison of overall survival rates between Group M (n=56) and Group N (n=54). Significant difference was observed between two groups (P=0.0034).

Fig. 2
Comparison of disease-free survival rate between Group M (n=56) and Group N (n=54). Significant difference was observed between two groups (P=0.0012).
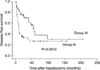
Table 1
Comparison of clinicopathologic variables between patients with hepatocellular carcinoma who met Milan criteria (Group M) and those who did not (Group N)






References
1. Omata M, Tateishi R, Yoshida H, Shiina S. Treatment of hepatocellular carcinoma by percutaneous tumor ablation methods: Ethanol injection therapy and radiofrequency ablation. Gastroenterology. 2004. 127:S159–S166.
2. Tateishi R, Shiina S, Teratani T, Obi S, Sato S, Koike Y, et al. Percutaneous radiofrequency ablation for hepatocellular carcinoma. An analysis of 1000 cases. Cancer. 2005. 103:1201–1209.
3. Shiina S, Teratani T, Obi S, Sato S, Tateishi R, Fujishima T, et al. A randomized controlled trial of radiofrequency ablation with ethanol injection for small hepatocellular carcinoma. Gastroenterology. 2005. 129:122–130.
4. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996. 334:693–699.
5. Adam R, Azoulay D, Castaing D, Eshkenazy R, Pascal G, Hashizume K, et al. Liver resection as a bridge to transplantation for hepatocellular carcinoma on cirrhosis: a reasonable strategy? Ann Surg. 2003. 238:508–519.
6. Cherqui D, Laurent A, Mocellin N, Tayar C, Luciani A, Van Nhieu JT, et al. Liver resection for transplantable hepatocellular carcinoma: long-term survival and role of secondary liver transplantation. Ann Surg. 2009. 250:738–746.
7. Cha CH, Ruo L, Fong Y, Jarnagin WR, Shia J, Blumgart LH, et al. Resection of hepatocellular carcinoma in patients otherwise eligible for transplantation. Ann Surg. 2003. 238:315–323.
8. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AJCC Cancer Staging Manual. 2002. 6th ed. New York: Springer.
9. Bigourdan JM, Jaeck D, Meyer N, Meyer C, Oussoultzoglou E, Bachellier P, et al. Small hepatocellular carcinoma in Child A cirrhotic patients: hepatic resection versus transplantation. Liver Transpl. 2003. 9:513–520.
10. Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Dennison A. Liver resection versus transplantation for hepatocellular carcinoma in cirrhotic patients. Ann Surg. 1993. 218:145–151.
11. Margarit C, Escartin A, Castells L, Vargas V, Allende E, Bilbao I. Resection for hepatocellular carcinoma is a good option in Child-Turcotte-Pugh class A patients with cirrhosis who are eligible for liver transplantation. Liver Transpl. 2005. 11:1242–1251.
12. Kang KT, Kim SB, Choi DW. Effects of partial hepatectomy for hepatocellular carcinoma meeting Milan criteria combined with compensated liver cirrhosis. J Korean Surg Soc. 2006. 71:189–196.
13. Tanaka S, Noguchi N, Ochiai T, Kudo A, Nakamura N, Ito K, et al. Outcomes and recurrence of initially resectable hepatocellular carcinoma meeting milan criteria: Rationale for partial hepatectomy as first strategy. J Am Coll Surg. 2007. 204:1–6.
14. Yamamoto J, Kosuge T, Saiura A, Sakamoto Y, Shimada K, Sano T, et al. Effectiveness of hepatic resection for early-stage hepatocellular carcinoma in cirrhotic patients: subgroup analysis according to Milan criteria. Jpn J Clin Oncol. 2007. 37:287–295.
15. Park YK, Kim BW, Wang HJ, Kim MW. Hepatic resection for hepatocellular carcinoma meeting Milan criteria in Child-Turcotte-Pugh class a patients with cirrhosis. Transplant Proc. 2009. 41:1691–1697.
16. Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999. 30:1434–1440.
17. Figueras J, Jaurrieta E, Valls C, Ramos E, Serrano T, Rafecas A, et al. Resection or transplantation for hepatocellular carcinoma in cirrhotic patients: outcomes based on indicated treatment strategy. J Am Coll Surg. 2000. 190:580–587.
18. Belghiti J, Cortes A, Abdalla EK, Regimbeau JM, Prakash K, Durand F, et al. Resection prior to liver transplantation for hepatocellular carcinoma. Ann Surg. 2003. 238:885–893.
19. Vennarecci G, Ettorre GM, Antonini M, Santoro R, Maritti M, Tacconi G, et al. First-line liver resection and salvage liver transplantation are increasing therapeutic strategies for patients with hepatocellular carcinoma and child a cirrhosis. Transplant Proc. 2007. 39:1857–1860.
20. Kaibori M, Saito T, Matsui Y, Uchida Y, Ishizaki M, Kamiyama Y. A review of the prognostic factors in patients with recurrence after liver resection for hepatocellular carcinoma. Am J Surg. 2007. 193:431–437.
21. Itamoto T, Nakahara H, Tashiro H, Ohdan H, Hino H, Ochi M, et al. Indications of partial hepatectomy for transplantable hepatocellular carcinoma with compensated cirrhosis. Am J Surg. 2005. 189:167–172.
22. Shah SA, Cleary SP, Wei AC, Yang I, Taylor BR, Hemming AW, et al. Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery. 2007. 141:330–339.
 XML Download
XML Download