

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several prospective randomized studies of laparoscopic surgery for colorectal cancer had shown both short-term benefits such as less pain, better cosmetic effect, faster recovery, and long-term oncological safety [12345]. So nowadays, laparoscopic surgery for colorectal cancer has been accepted as an alternative to conventional open surgery. So many colorectal surgeons have considered laparoscopic surgery as a useful surgical tool for treatment of colorectal cancer. However, conventional multiport laparoscopic surgery (CMLS) for colorectal cancer requires 4 or 5 abdominal incisions for trocars and each incision could be associated with wound complications and pain. Single port laparoscopic surgery (SPLS) permits surgeons to reduce such wound related complications and achieve better cosmetic effects compared to CMLS. The potential advantages of SPLS are less pain and earlier recovery than CMLS. Actually, several studies had already reported acceptable short-term outcomes of SPLS compared to CMLS [6789]. However, SPLS is a highly demanding procedure that also has several technical challenges such as handling conventional laparoscopic instruments through small incisions, which could decrease the range of motion; and, there could be conflict between instruments and camera. As a result, there are also potential disadvantages such as longer operation time, increased surgeon fatigue and steep learning curve.
Reduced port laparoscopic surgery (RPLS), which is single port plus one additional port, may overcome the limitations of SPLS while maintaining the advantages of SPLS.
The aim of this study is to evaluate the short-term outcomes of RPLS and assess the safety and feasibility of RPLS in colon cancer.
METHODS
This study is a retrospective review of prospectively collected data of patient who underwent CMLS and RPLS for colon cancer between August 2011 and December 2013 at Incheon St. Mary's Hospital, The Catholic University of Korea by a single surgeon. All patients underwent preoperative work-up including colonoscopy with biopsy, CT, laboratory test, and chest radiography. All patients with colorectal cancer admitted to Incheon St. Mary's Hospital were considered for laparoscopic surgery, both CMLS and RPLS. Because of the nature of the retrospective study, the indication for RPLS for colon cancer was not so strict and changed case by case. In general, patients with ascending or sigmoid colon cancer with small sized tumor and relatively early stage were considered for RPLS. In our institute, rectal cancer and transverse colon cancer were also considered for laparoscopic surgery. However, in this study, rectal cancer and transverse colon cancer were excluded; because, in our institute, rectal cancer and transverse colon cancer were only considered for CMLS but not for RPLS or SILS. Informed consent was obtained from all patients. In our institute, critical pathway was used for all patients who underwent colorectal cancer surgery. In the present study, we compared short-term clinical outcomes including pain score and pathologic outcomes between CMLS and RPLS. Postoperative pain was categorized into 0–3; 0 (no pain), 1 (mild pain), 2 (moderate pain), 3 (severe pain). And pain level was checked at 2:00 PM on postoperative day 1, 3, and 5. In our institution, we routinely use patient-controlled analgesia (PCA), with a regimen containing fentanyl. But in case where patients refuse PCA, we use continuous infusion combined with bolus injection of pethidine hydrochloride. We analyzed the total amount of infused analgesics as converted into fentanyl (fentanyl 1,000 µg was considered equal to 750 mg of pethidine).
This study was approved by the Institutional Review Board of Incheon St. Mary's Hospital (OC14RISI0087).
Operative procedure
For both CMLS and RPLS, patients were placed in the lithotomy position. For CMLS, a 10-mm trocar was inserted at umbilicus for the camera, and 4 trocars were inserted at RLQ (right lower quadrant), RUQ (right upper quadrant), LLQ (left lower quadrant), and LUQ (left upper quadrant) sites. For RPLS, a single port was inserted using transumbilical incision and an additional port insert in the dominant-hand side of the operator (Fig. 1). All RPLS were performed using an OCTO port (Dalim SurgNET, Seoul, Korea), single port with a 4-channel system. For right colon cancer, we performed complete mesocolonic excision (CME) and central vessel ligation (CVL) independent to tumor stages in both RPLS and CMLS. For sigmoid colon cancer, high ligation of inferior mesenteric artery was routinely performed in both RPLS and CMLS. In RPLS of anterior resection, proximal rectal transection was performed using a linear stapler, which was introduced via additional RLQ port, and intracorporeal stapled anastomosis was performed. For right hemicolectomy, extracorporeal resection and anastomosis was performed. In RPLS, all the specimens were retrieved through the single port and in CMLS, all specimens were extracted through extension of the umbilical incision. After anastomosis, irrigation was done in the abdominal cavity and a drain was inserted through the port incision.
RESULTS
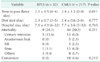
During the study period, 32 cases were enrolled in RPLS group and 217 cases were enrolled in CMLS group. In the present study, no significant differences were shown in terms of demographics and clinical characteristics of patients between the 2 groups (Table 1). In terms of operative outcomes, longer operation time and large amount of blood loss were shown in CMLS group (Table 2). In terms of pathological outcomes, tumor size and harvested number of lymph nodes were larger in CMLS group compared to RPLS group. When we compared the pathologic tumor stage, stage I was more frequent in RPLS group and stages II and III were more frequent in CMLS group. The rate of stage IV was similar between the 2 groups.
In terms of postoperative clinical outcomes, time to pass flatus was shorter in RPLS group compared to CMLS (2.1 ± 0.9 vs. 2.4 ± 1.3, P = 0.011) (Table 3). Surgical morbidity was 9 cases (28.1%) in RPLS group and 44 cases (20.3%) in CMLS group. Anastomosis leak was encountered in 0 cases in RPLS group and 5 cases in CMLS group but showed no difference. And in terms of conversion, there was no significant difference. There was no surgical mortality in this study.
In the present study, we estimated postoperative pain between the 2 groups using numeric rating scale (NRS). NRS was significantly different between RPLS and CMLS. NRS of RPLS at postoperative day (POD) 1, 3, and 5 were significantly lower than those of CMLS (Table 4). There was no significant difference in terms of total amount of infused analgesics.
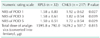
In subgroup analysis of stage I colon cancer, pathologic outcomes such as PRM, DRM, or harvested lymph nodes did not differ between the 2 groups (Table 5). A shorter operative time was observed in the RPLS group. However, in terms of postoperative pain, only the NRS score of POD 3 was significantly lower in the RPLS group than the CMLS group.
DISCUSSION
During the past decades, several large prospective randomized trials have demonstrated better short-term clinical outcomes of laparoscopic surgery for colorectal cancer, and also established the long-term oncological safety of laparoscopic surgery for colorectal cancer [1011121314]. So nowadays, many surgeons consider laparoscopic surgery as a better surgical option to treat patients suffering from colorectal cancer than conventional open surgery.
However, conventional laparoscopic surgery requires 3 or more ports and also need an additional incision for specimen removal. Additionally, each trocar site incision has potential risk for morbidities such as postoperative wound pain and negative effects on cosmetic outcomes. Accumulation of experience in advanced laparoscopic surgery combined with development of laparoscopic surgical instruments has induced to use less trocars or single trocar. Many surgeons had applied single incision laparoscopic surgery to the era of colorectal cancer expecting potential advantages including better cosmetic outcomes, less postoperative pain, and faster recovery, and several studies have reported such short-term outcomes [151617].
However, single incision laparoscopic surgery is technically difficulty and results in increasing surgeon fatigue and operation time compared to CMLS [181920].
RPLS, a single port with one additional port, may decrease the technical difficulties of SILS while maintaining its cosmetic outcomes and can be consider as a bridge to SILS. However, there are few studies evaluating the safety or technical feasibility of RPLS.
In the present study, 7 cases of low anterior resection for distal sigmoid colon cancer were enrolled in RPLS group. Although the safety and technical feasibility of SILS low anterior resection has been reported [2122], until now those factors had not yet been established. Actually, applying laparoscopic linear stapler through a single port for rectal transection does not permit sufficient distal resection margin and is sometimes physically and technically impossible in a narrow pelvis. Inserting an additional port at RLQ permits the surgeon to apply a laparoscopic linear stapler and perform rectal transection more easily.
One of the disadvantages of SILS for colon cancer is longer operation time compared to conventional laparoscopic multiport surgery [2324]. There are several possible explanations for the longer operation time of SILS. The most important reason is limitation of motion and reduced ability of triangular dissection. Because a camera and 2 laparoscopic instruments are introduced into the peritoneal cavity through a small incision or the umbilicus, collision and conflict between the camera and laparoscopic instruments are inevitable. Also, the steep learning curve of SILS is another possible explanation. Inserting one additional port at the surgeon's dominant-hand side might resolve those drawbacks of SILS, including collision and difficulty of triangular dissection. Several studies of RPLS reported that operation time of RPLS was comparable to CMLS [2526]
In the present study, the operation time was significantly shorter in RPLS group compared to CMLS group. We considered it as selection bias; because tumor size was also significantly smaller and tumor stage I was significantly more frequent in RPLS group. However, in the subgroup analysis for stage I cancer, the operation time of RPLS was significantly shorter than CMLS group. Another reason for shorter operative time of RPLS might be caused by the operator's advanced techniques. CMLS was generally performed earlier during the study period than RPLS, therefore the surgeon's technique might have improved with the passage of time. In our institute, the extent of surgery was the same, independent of tumor stage; CME and CVL for right colon cancer and high ligation of inferior mesenteric artery for sigmoid colon cancer. So, considering difference of tumor stage, we thought operation time of RPLS for colon cancer was comparable to CMLS for colon cancer.
When introducing a new surgical technique, intraoperative morbidity and postoperative morbidity are very important issues. And one of the parameters of intraoperative morbidity is the amount of intraoperative blood loss. In the present study, blood loss during surgery was about 24 mL in RPLS group and 56 mL in CMLS group, which showed statistical difference. And in terms of postoperative morbidities, there were no significant difference between the 2 groups. Anastomosis leakage is one of the most dreadful complications of colorectal surgery and could result in severe surgical morbidity or mortality. Although it is still controversial, reducing the number of linear stapler firings was necessary to avoid anastomosis leakage after laparoscopic colorectal surgery [27]. During SILS anterior or low anterior resection, applying a linear stapler and proximal rectum transection is a very challenging procedure. Sometimes more linear staplers are needed, because it is difficult to achieve the right angle between the bowel and linear stapler. Using one additional port for the linear stapler permitted the surgeon to transect the proximal rectum easier. In the present study, authors used an average of 1.3 linear staplers in anterior resection and 2.0 in low anterior resection, and there was no anastomosis leakage in RPLS group. Authors thought that insertion of an additional port could reduce the number of linear staplers for anterior or low anterior resection, and also risk of anastomosis leakage.
In terms of postoperative recovery, time to pass flatus of this study was shorter in RPLS group compared to CMLS group. The authors used the same critical pathway for all patients who underwent laparoscopic colorectal cancer surgery in both RPLS and CMLS. We thought less postoperative pain contributed to faster bowel movement because if the patients had less postoperative pain, earlier ambulation could be possible resulting in faster bowel movement.
When single incision laparoscopic surgery was introduced, many surgeons expected potential advantages, especially less postoperative pain compared to CMLS. However, that potential advantage is still controversial and several studies have reported that postoperative pain of SPLS was similar to or more severe than CMLS [282930]. The authors thought that although SPLS has the advantage of a single incision, this single incision site might be strongly lengthened and stretched by inserting a single port during the operation since SPLS has several technical challenges such as handling conventional laparoscopic instruments. So, that could be the major cause of postoperative pain of SILS.
The advantages of RPLS are a relative decrease of technical difficulties of SILS while maintaining cosmetic outcomes of SILS, and comparable operation time compared to CMLS.
Therefore, the single incision site of RPLS is less lengthened and stretched than that of SPLS during operation and the lengthening and stretching time of the single incision site of RPLS is shorter than that of SPLS. These factors can explain why patients who underwent RLPS could experience less pain. However, there are few studies evaluating the postoperative pain of RPLS and reported favorable result. In the present study, we evaluated postoperative pain of RPLS group and CMLS group using NRS. Although authors used the same critical pathway for all patients, NRS of RPLS at POD 1, 3, and 5 were significantly lower than those of CMLS. We assumed that relative decrease of technical difficulties and shorter operation time of RPLS contributed to less postoperative pain.
There were several limitations in this study. First, this study is retrospective and has selection bias. We performed RPLS in the relatively early stage of colon cancer compared with CMLS. Second, this study did not compare the cosmetic outcomes or patient satisfaction of cosmetic effects. Large-scale prospective randomized studies are needed to establish the benefits of RPLS in colon cancer.
In conclusion, the present study showed that RPLS for colon cancer is safe and technically feasible. And in terms of postoperative pain, RPLS was more favorable than CMLS. We thought RPLS for colon cancer could be a good surgical option for selected patients suffering from colon cancer.




 XML Download
XML Download