

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neoadjuvant concurrent chemoradiotherapy (NCRT) has become the standard therapeutic strategy for locally advanced rectal cancers owing to its benefit in terms of improving local control, increasing resectability, and reducing toxicity despite no impact on overall survival [123]. However, chemotherapeutic regimen has not been standardized. The Mayo regimen has been used as chemotherapy in many major studies [123] and continues to be widely used. In this regimen, patients are intravenously administered 5-fluorouracil (5-FU) and leucovorin for 5 days at the first and fifth weeks of concurrent 6-week radiotherapy (RT). Although 5-FU does not typically induce severe side effects, this treatment regimen is invasive and can result in complications related to injection. This can decrease treatment compliance and consequently affect the patient's oncologic outcome. Oral capecitabine is another option for NCRT: patients take capecitabine twice a day during 6 weeks of RT. This treatment modality mimics continuous infusion [4], is easy to administer, and is patient-friendly because it does not involve injection or admission. Many studies have reported on the improved safety of capecitabine-based NCRT [56]; however, only a few studies have evaluated its long-term oncologic outcomes [78]. If the oncologic outcomes of capecitabine are not inferior to those of the Mayo regimen, capecitabine would be the drug of choice for NCRT in rectal cancers. Our institute has used capecitabine as part of the NCRT regimen for more than 10 years. Herein, we report the long-term oncologic outcomes and prognostic factors of patients who received capecitabine as NCRT along with radical surgery.
METHODS
Patients
From January 2000 to June 2010, 266 patients were treated for advanced rectal cancer using capecitabine-based NCRT. As using the electronic medical records system retrospectively, their clinical and pathologic data were collected. Inclusion criteria were as follows: (1) histologically confirmed adenocarcinoma within 12 cm from the anal verge; (2) locally advanced disease (stage T3, T4 or node-positive disease) without distant metastasis confirmed with radiologic examination; (3) conventional NCRT with capecitabine followed by a 6-week resting period; (4) radical resection performed with total mesorectal excision. Among 13 patients with distant metastases diagnosed before or after the NCRT, 4 patients who were administered chemotherapy according to the Mayo regimen, 3 patients whose resting periods were extremely long because of initial refusal to undergo operation, 6 patients who underwent local excision, and 2 patients who underwent palliative resection were excluded. The final analysis included 238 patients.
Evaluation and treatment protocol
Initial evaluation consisted of complete history-taking, physical examination including digital rectal examination, colonoscopy or alternative proctoscopy when passing the scope through the tumor was impossible, complete blood count, serum biochemistry, CEA level, chest radiography, abdominopelvic CT, basically. At least one examination of endorectal ultrasonography and rectal MRI was performed, and PET/CT was performed selectively. Patients were classified as having lower (≤4 cm from the anal verge), middle (4–8 cm), or upper (8–12 cm) rectal cancer according to the location of the tumor. Postneoadjuvant treatment evaluation was performed at the end of the resting period and consisted of digital rectal examination, flexible sigmoidoscopy, complete blood count, serum biochemistry, CEA level, abdomino-pelvic computed tomography CT, and rectal MRI.
RT and chemotherapy was initiated simultaneously and delivered to the whole pelvis using a three-field approach at a total dose of 50.4 Gy, using conventional fractionation (daily fractions of 1.8 Gy over 6 weeks, excluding weekends). The RT target included the entire tumor with a margin of more than 5 cm, the mesorectum, and the iliac and presacral lymph nodes up to the L5–S1 junction. Oral capecitabine was administered at a dose of 825 mg/m2 twice daily for 6 weeks concomitantly with RT. The intended duration of the resting period (completion of NCRT to surgery) was 6 weeks, and modulation within several weeks was permitted flexibly considering the patient's condition and situation. Radical surgery including low anterior resection, intersphincteric resection, or abdominoperineal resection was performed according to the protocol for total mesorectal excision. En bloc resection was performed when adjacent organ invasion was suspected, and lateral pelvic lymph node dissection was performed when metastasis was suspected at the preoperative, radiologic examination. Loop ileostomy for transient diversion was performed when surgeons decided it was necessary, but not routinely. Adjuvant chemotherapy is generally started from postoperatively 2 weeks to 2 months based on the NCCN guideline that postoperative therapy is indicated in all patients who receive preoperative therapy, regardless of the surgical pathology results.
Study assessment and surveillance
Toxicity was assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 [9]. Postoperative complications were assessed according to the Clavien-Dindo classification [10]. Pathological evaluation of the surgical specimen was performed by expert pathologists. The pathological response of the tumor was determined using the College of American Pathologists (CAP) scale: grade 0, complete disappearance of all tumor cells (pathologic complete response [pCR]); grade 1, single cells or small groups of cancer cells (moderate response); grade 2, residual cancer outgrown by fibrosis (minimal response); grade 3, minimal or no tumor response and extensive residual cancer (poor response). Postoperative surveillances were performed 2 months after the operation, then every 4 months for 2 years, and every 6 months for the next 3 years. The modality of evaluation included complete blood count, serum biochemistry, CEA level, chest radiography, and abdominopelvic CT. If a patient required further evaluation due to suspected recurrence on the basis of the findings from the above-mentioned examination, chest CT, liver MRI, rectal MRI, or PET/CT was performed accordingly. Colonoscopy was performed 1 year after the operation, and the schedule thereafter was tailored according to each patient's condition.
Statistical analysis
Data regarding clinical and pathologic characteristics were collected retrospectively, and the capecitabine-related toxicity and postoperative complications were reviewed. Five-year overall survival, 5-year disease-free survival, local recurrence, and systemic recurrence were estimated using Kaplan-Meier analyses. Univariate and multivariate analyses to evaluate factors associated with oncologic outcomes were performed with the log rank and Cox regression tests. IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) was used for the statistical analysis. The study was approved by the Institutional Review Board of the institute Chungnam National University Hospital (approval number. 2016-08-053).
RESULTS
The clinical and pathologic characteristics of the patients are presented in Table 1. The pCR rate was 14.7% (n = 35). All except for 3 patients were administered adjuvant chemotherapy: 221 received oral chemotherapy with doxifluridine, uracil/tegafur, or capecitabine and 14 patients received intravenous chemotherapy with Mayo, FOLFOX (Oxaliplatin, 5-fluorouracil), FOLFIRI (Irinotecan, 5-fluorouracil), CapeOx (Capecitabine, oxaliplatin) or CapeIRI (Capecitabine, irinotecan).
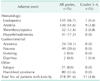
Episodes of capecitabine-related toxicity, according to the CTCAE version 4.0, are presented in Table 2. According to the CTCAE version 4.0, we defined leukopenia, anemia, and thrombocytopenia as a WBC count below 4,500 cells/mm3, hemoglobin level below 12.0 g/dL, and platelet count below 130,000 cells/mm3. Although a significant number of patients were classified as having leukopenia (n = 153) and anemia (n = 130) and one and nine of them were showed grade 3 (1,000 < WBC < 2,000 cells/mm3 and hemoglobin < 8.0 g/dL) after a retrospective review of laboratory results, no patients demonstrated any adverse clinical conditions except for packed red blood cell transfusion. The incidence of hand-foot syndrome was 33.6% (n = 80), and the incidence of toxicity grade >3 (severe skin changes [e.g., peeling, blisters, bleeding, edema, or hyperkeratosis] with pain; limiting self-care activities of daily living [ADL]) was 4.6% (n = 11). Only one patient needed to be admitted for conservative treatment owing to capecitabine-induced diarrhea of grade 3 (Increase of ≥7 stools per day over baseline; incontinence; hospitalization indicated; severe increase in ostomy output compared to baseline; limiting self-care ADL), and he was the only patient who had to discontinue receiving capecitabine.
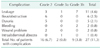
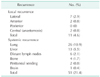
Postoperative complications, according to Clavien-Dindo classification, are presented in Table 3. The incidence of anastomotic leakage was 4.6% (n = 11), and the incidence of grade >2 complications was 11.3% (n = 27). The median follow-up period was 78.7 months. The 5-year overall and 5-year disease-free survival rate, local and systemic recurrence rate estimated using Kaplan-Meier analyses were 82.8%, 75.1%, 4.8%, and 20.3% (Fig. 1). The patterns of local and systemic recurrences are shown in Table 4. The most common site of local recurrence was the lateral pelvic nodes (2.9%, n = 7), and the most common site of systemic recurrence was the lungs (10.9%, n = 26).
In the univariate analyses, the operation method, pN stage, tumor size, and lymphatic and vascular invasion were significantly associated with 5-year overall survival. Age, operation method, pT stage, pN stage, tumor size, lymphatic and vascular invasion were significantly associated with 5-year disease survival. No factor was significantly associated with 5-year local recurrence. Age, operation method, pT stage, pN stage, and lymphatic and vascular invasion were significantly associated with 5-year systemic recurrence (Table 5). In the multivariate analyses, the operation method and pN stage were independent prognostic factors for 5-year overall survival, 5-year disease-free survival, and systemic recurrence (Table 6).
DISCUSSION
Owing to the development of surgical techniques, chemotherapy, and multimodality therapy, the oncologic outcomes of locally advanced rectal cancer have significantly improved. Previous studies regarding NCRT for locally advanced rectal cancer have reported a 5-year survival of 65.2%–76%, 5-year disease-free survival of 52.2%–68%, 5-year local recurrence rate of 6%–10.7%, and 5-year distant recurrence rate of 34.4%–36% [12311]. Recently, Lange et al. [12] reported a 5-year overall survival of 76.4%, local recurrence rate of 5.2%, and distant recurrence rate of 22.1%, which is rather encouraging.
In many studies including the above-mentioned studies, intravenous 5-FU was used for neoadjuvant chemotherapy. However, there is a lack of literature regarding the long-term oncologic outcomes of NCRT with capecitabine.
Capecitabine
Capecitabine (Xeloda, Hoffmann-LaRoche Inc., Nutley, NJ, USA) is an orally bioavailable fluoropyrimidine that generates 5-FU by thymidine phosphorylase, which is produced in large amounts in tumor tissues [13]. The administration of capecitabine resulted in higher concentrations of 5-FU in tumor tissue and lower concentrations in normal tissue in vivo, compared with bolus or continuous intravenous 5-FU [14]. One preclinical study reported that the antitumor effect of capecitabine was superior to that of 5-FU in human cancer xenograft models [15]. The oncologic noninferiority of capecitabine was improved in an adjuvant setting for stage III colorectal cancers [16] and also a palliative setting for stage IV colorectal cancers [17]. Sawada et al. [18] reported that RT up-regulated the expression of thymidine phosphorylase and enhanced the effect of capecitabine in tumor tissue, but did not show any clear additive effects after RT with intravenous 5-FU. They insisted that RT with capecitabine would have greater efficacy than conventional RT with intravenous 5-FU. Capecitabine in NCRT has tolerable toxicity and a considerable downstaging effect [5], and equivalent 3-year oncologic outcomes compared with intravenous 5-FU have been reported [19]. Hofheinz et al. [6] conducted a randomized trial using 2 cohorts administered neoadjuvant and adjuvant therapy, and reported noninferior 3-year overall survival, disease-free survival, and local recurrence rate, but superior 3-year distant metastasis rate for capecitabine compared to intravenous 5-FU. Capecitabine is an attractive regimen for NCRT owing to its convenience and efficacy, and because it mimics continuous infusion and could potentially replace intravenous 5-FU [4]. However, there is a lack of data regarding the long-term oncologic outcomes for homogenous groups of patients treated using NCRT with capecitabine; therefore, we conducted the present study.
In our institution, capecitabine has been used as NCRT for locally advanced rectal cancers since 1999. Initially, it was administered in 2 cycles and each cycle lasted 2 weeks. According to an accumulation of experiences regarding its safety and efficacy, the schedule was standardized as follows: daily administration during 6 weeks of concurrent RT followed by a resting period of more than 6 weeks before radical surgery.
Oncologic outcomes
In the present study, oncologic outcomes were found to be favorable with the additional benefit of good tolerance and excellent compliance, when compared to other studies reporting the prognosis of NCRT and radical surgery. In terms of short-term oncologic results, the incidence of pCR was 14.7%, which was within the generally reported range [20]. There is a possibility that the pCR rate was overestimated in studies regarding NCRT that did not exclude cases with wait and see or local excision. This study excluded the above-mentioned cases completely, and therefore, the accuracy of pCR rate is reliable. Additionally, in every aspect of oncologic outcomes including overall survival, disease-free survival, local recurrence, and systemic recurrence rate, the results based on an adequate follow-up period (mean, 78.7 months) were relatively and significantly favorable, compared with several other studies.
Most recently, numerous studies reported short and long-term results of NCRT with combination of capecitabine, oxaliplatin, or bevacizumab. However, in many of those studies, the oncologic results were found to be not superior [2122], and more significant toxicity and inferior compliance were reported, on the contrary [23]. Further research will be necessary to confirm that above-mentioned combinations of treatments could obtain more improved prognosis. However, up to the present time, it is considered that NCRT with capecitabine alone can produce not inferior oncologic outcomes safely and patient-friendly, compared with any other type of treatment.
Safety
In terms of safety, capecitabine was well tolerated, with 4.6% of cases of toxicity above grade 3 and tolerable drug compliance with only 1 patient who did not complete the schedule owing to grade 3 diarrhea. The rates of total hematologic toxicity were significantly high; however, almost all cases were subclinical. The most common type of clinical toxicity was hand-foot syndrome (33.6%), which is known as the representative side effect of capecitabine; however, no patient experienced grade >3 evens, and all symptoms improved without special treatment. It is well known that patients administered capecitabine experience significantly less diarrhea, nausea, vomiting, neutropenia, but more hand-foot syndrome than those administered intravenous 5-FU [24]. The rate of hand foot syndrome in patients treated with capecitabine has been reported as high as 45%–56% [25]. However, most cases of capecitabine-induced hand foot syndrome are tolerable and self-limited; these cases are never life-threatening, and can be easily managed by patient education, treatment interruption, or dose reduction, and rarely results in treatment discontinuation or hospitalization [26]. Consequently, capecitabine can be safe and effective choice of therapeutic strategy especially in elderly patients who are inappropriate to receive intravenous chemotherapy [27].
The rates of postoperative complication were also in the average range generally reported. Therefore, capecitabine was not considered to increase the rates of postoperative complications.
Prognostic factors
According to the multivariate analyses of the present study, abdominoperineal resection (APR) and node-positive disease were independently significant prognostic factors for overall survival, disease-free survival, and systemic recurrence rate. APR is a well-known prognostic marker for local recurrence and survival [28], even in patients with a clear circumferential resection margin [29]. Pathologic N stage is known as the most important factor for oncologic outcomes [30]. However, in the present study, any prognostic factor did not have a statistically significant correlation to local recurrence. For this reason, we supposed that the difference in local recurrences between each subgroup was insignificant to compare because the total local recurrence rate was already low at 4.6%.
Limitations
There are limitations in the present study. Because this is a noncomparative, retrospective study, although we reported the favorable oncologic results of capecitabine, its superiority cannot be improved. Secondly, there is heterogeneity in terms of the adjuvant chemotherapy, especially in the early part of the studied period. There was no national or universal guideline for adjuvant chemotherapy of rectal cancer, and there had been many changes of recommendation in both fields of medicine and ministerial policy. However, the principle that locally advanced rectal cancers require adjuvant therapy even after down-staging after NCRT was applied to most cases as observing the NCCN guideline. A prospective, randomized study with control of adjuvant chemotherapy is necessary to obtain more solid evidence about the oncologic superiority of capecitabine compared with other treatments.
In conclusion, based on that NCRT with capecitabine and radical surgery showed favorable long-term oncologic outcomes with benefits of acceptable toxicity and convenience, we suggest that capecitabine can be one of the favorable therapeutic options for NCRT in rectal cancer.




 XML Download
XML Download