

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of food allergy (FA) varies in different countries, as estimates are affected by many factors, such as age, ethnicity, frequency of dietary exposure, and cooking method.12 In addition, methodology, type of FA, and the size of the study population also influence the results of the epidemiologic studies. 3 Among US children, the prevalence of self-reported FA in 2007-2010 was 6.53%, while 7.1% of Canadian children had FA in a telephone survey conducted between 2008 and 2009.45 The pooled prevalence of self-reported FA in Europe was 6.9% in children aged 0-17 years.6 In Taiwanese children aged 4-18 years, the overall prevalence of FA was 7.65%, while the prevalence of FA among 0-14-year-old Hong Kong children in 2005-2006 was 4.8%.78 In Japan, the FA prevalence was estimated as 5%-10% in 0- to 6-year-old children and 1%-2% in 6- to 15-year-old children.9 These data demonstrate geographical differences in FA prevalence.
In Korea, nationwide epidemiologic studies on FA in the general population were performed in 1995 and 2000, as part of the International study of Asthma and Allergies in Childhood (ISAAC). In the ISAAC, the prevalence of children ever diagnosed with FA in 6- to 12-year-olds was 4.2% in 1995 and 4.7% in 2000, while the prevalence of FA in 13- to 15-year-olds was 3.8% in 1995, increasing to 5.1% in 2000.10 Despite the large sample size of over 40,000, the diagnostic accuracy was limited because the diagnosis relied on parental report. Since then, the prevalence of immediate-type FA in the general population has been calculated using an algorithm involving detailed history, such as symptoms, time elapsed after specific ingestion, and repetitiveness. In a 2006 birth cohort study evaluating 1,177 infants, the prevalence of immediate-type FA was 5.3%, and the leading causes were hen's egg, cow's milk, peanut, and tree nuts.11 In a 2010 nationwide survey, the prevalence of immediate-type FA was estimated as 2.0% in 6- to 7-year-olds and 3.6% in 12- to 13-year-olds.12 Among 16,749 children aged 0-6 years, the prevalence of immediate-type FA was 3.7%.13
Avoidance of the offending food is important in the management of FA, especially in schoolchildren, because they are served meals through a school lunch program. Although several guidelines have been proposed for FA management in schools, minor allergic reactions and food-induced anaphylaxis have still occured.14 FA also has a negative influence on quality of life.15 In particular, schoolchildren are in a critical time for growth spurts and emotional changes. In daily nutrition intakes, patients with FA have a fear of allergic reactions and experience social isolation and depression.1617 As a result, FA can affect a child's development and can be a potential problem among family members and friends.15
In the present study, we investigated the prevalence of immediate-type FA and common causes among Korean schoolchildren in a nationwide, cross-sectional, questionnaire survey conducted in 2015. This study provides information about one of the important health problems in schoolchildren and also helps expand our understanding of the current status of FA in Korean children and adolescents.
MATERIALS AND METHODS
Study population
This nationwide, cross-sectional, population-based epidemiologic study was conducted in Korea, in September 2015. Our study population included schoolchildren in 4 age groups of 6-7, 9-10, 12-13, and 15-16 years. Participants in this survey were selected by a 2-stage stratified random sampling design. For the first stage, schools across the country were stratified by geographic region and school type. Geographic regions were classified into 17 cities and provinces according to administrative district. School types were divided into elementary schools, middle schools, and high schools. From each stratum, sample schools were selected by the systematic probability proportional to size (PPS) sampling method. For the second stage of sampling, one class was selected randomly from each sample school. Across the nation, a total of 50,000 children were randomly chosen. In this study, 35,000 children in the first and fourth grades of 500 elementary schools (6- to 7 and 9- to 10 years-olds), 7,500 children in the first grade of 250 middle schools (12- to 13 years-olds), and 7,500 children in the first grade of 250 high schools (15- to 16 years-olds) were selected. This study was approved by the Institutional Review Board at Samsung Medical Center, Seoul, Korea (IRB No. 2015-07-204-002).
Definition of FA and anaphylaxis
Current immediate-type FA was defined according to an algorithm that included a detailed history of immediate-type FA (Fig. 1). When the parents answered “yes” to the question “Has your child ever had allergic reactions to foods,” their children were considered as having “perceived FA, ever.” Among those who have “perceived FA, ever,” children with common allergic reactions within 4 hours after ingestion of the suspected food were chosen. Common allergic symptoms included skin or mucosal symptoms (urticaria, itching, aggravated eczema, facial edema, eyelid edema, and lip edema), respiratory symptoms (cough, rhinorrhea, wheezing, dyspnea, and cyanosis), gastrointestinal symptoms (vomiting, diarrhea, and abdominal pain), and cardiovascular symptoms (hypotension, altered mentality). Children with only 1 vague symptom, such as vomiting, diarrhea, or itching, were excluded. If children repeatedly manifested allergic reactions or never ate that food again, we determined that they had “immediate-type FA, ever.” If children still restricted ingestion of the suspected food at the time of the survey, they were regarded as having “immediate-type FA, current.” The diagnosis of anaphylaxis was defined according to the criteria proposed in the second symposium on the definition and management of anaphylaxis.18
In the questionnaires, parents were asked to choose suspected foods among individual food items (hen's egg, cow's milk, soy, peanut, wheat, buckwheat, beef, chicken, pork, sesame, and others) and food groups (tree nuts, fruits, vegetables, fishes, and crustaceans).
Statistical analysis
Because the population for this study was selected using a stratified 2-stage random sampling design, we calculated the sampling weights to consider differential selection probabilities, non-response, and post-stratification adjustments. Data were analyzed using SPSS version 23.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Questionnaires from 32,001 of 50,000 participants (64.0%) were completed. After adjustment for missing data, data from 29,842 children (59.7%) were included in the final analyses. This survey included 9,671 children aged 6-7 years, 9,756 children aged 9-10 years, 5,169 children aged 12-13 years, and 5,246 children aged 15-16 years. The demographic data are shown in Table 1.
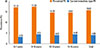
The overall prevalence of perceived FA was 15.82%, and that of current immediate-type FA was 4.06% (Fig. 2). According to age, the prevalence of immediate-type FA was 3.15% in 6- to 7-year-olds, 4.51% in 9- to 10-year-olds, 4.01% in 12- to 13-year-olds, and 4.49% in 15- to 16-year-olds.
Peanut was the most frequent causative food of current immediate-type FA, with a prevalence of 0.22%, followed by hen's egg (0.21%), cow's milk (0.18%), and buckwheat (0.13%) (Fig. 3). Causative foods differed according to age (Table 2). Hen's egg was the most common cause in 6- to 7-year-olds, whereas peanut, cow's milk, and buckwheat were reported to be the most frequent cause in 9-to 10-year-olds, 12-to 13-year-olds, and 15- to 16-year-olds, respectively. Among the food groups, fruits (1.41%) were the most frequent causes of allergy, followed by crustaceans (0.84%), tree nuts (0.32%), and fish (0.32%) (Fig. 3). These frequencies were similar among different age groups (Table 2).
Skin or mucosal reaction was reported as the most common symptom (94.3%) of current immediate-type FA in schoolchildren, followed by respiratory symptoms (16.3%) and gastrointestinal symptoms (13.3%). Anaphylaxis was found in 22.5% of children with current immediate-type FA.
The overall prevalence of food-induced anaphylaxis was 0.97% in Korean schoolchildren. The most common causative food was peanut, with a prevalence of 0.08%, followed by cow's milk (0.07%), buckwheat (0.06%), and hen's egg (0.06%) (Fig. 4). Among the food groups, fruits (0.28%), crustaceans (0.18%), tree nuts (0.12%), and fish (0.09%) were frequent causes of food-induced anaphylaxis (Fig. 4).
DISCUSSION
The strength of our study is its large, nationwide probability sample; 29,842 schoolchildren participated in the present study, larger than most of the previous FA prevalence studies.2419 In addition, we used a 2-stage stratified random sampling design and selected study participants who represent all Korean schoolchildren in order to avoid selection bias. Instead of using parental report for the diagnosis of FA, we overcame this limitation of diagnostic accuracy by defining immediate-type FA through an algorithm of detailed history. Consequently, we obtained more objective FA data from a large study population representative of schoolchildren nationwide.
Although peanut and tree nuts have been considered common causes of FA in the Western world, the prevalence of peanut and tree nut allergy is relatively low among children in Asia. The prevalence rates of peanut allergy in schoolchildren were 0.22% in the present study, 0.43% in Philippines, and 0.47% in Singapore, while they were reported as 1.03%, 1.50%, and 1.40%, respectively in Canada, the United Kingdom, and the United States.202122 Similarly, the prevalence rates of tree nut allergy were 0.32% in the current study and 0.30% in Singapore, whereas they were 1.10% in the US and 1.67% in Australia.202223 Although direct comparisons between the countries are not possible due to the differences in the size of the study population and methodologies for diagnosing FA, the prevalence appears to vary between Asian and Western countries. Different prevalence rates of filaggrin loss-of-function mutation and atopic dermatitis might make the differences in the prevalence of peanut and tree nut allergies.2425 Another possible reason for the higher prevalence of peanut allergy in Western countries might be the exposure to peanuts with higher allergenicity, strict avoidance of peanut ingestion during infancy, or higher environmental peanut exposure.2627 Even though the exact mechanism is unknown, further investigation is required to prevent the development of peanut or tree nut allergy, which is increasing in Western countries.2228
Hen's egg and cow' milk are well-known causative foods of FA in many countries.121213 Most cow's milk and hen's egg allergies develop in the first year of life and are outgrown by early to late childhood.2930 However, recent studies have demonstrated that tolerance induction of hen's egg or cow's milk allergy is slower than previously described.313233 For example, approximately half of patients with hens' egg allergy reached tolerance by 12 years of age and the allergy persisted into late adolescence in 42%.31 Twenty-one percent of patients with a cow's milk allergy had not developed tolerance by the age of 16.32 In the current study, cow's milk and hen's egg were found to be the second and third most common food allergens in schoolchildren, which appear to reflect the late acquisition of oral tolerance in both allergies.
Among the food groups, fruit was the most frequent food allergen in the present study. Fruit allergy is generally caused by a variety of proteins cross-reacting with pollens, particularly from birch, ragweed, or mugwort. Because the pollen sensitization rate in Korean schoolchildren is 0.3%-10.1% and might be increasing due to climate change and air pollution, it is noteworthy to monitor whether fruit allergy in Korean children increases in the future.3435 Crustaceans are also common allergens. The prevalence of shellfish allergy among 14- to 16-year-old children was 5.12% in the Philippines and 5.23% in Singapore,20 whereas it was 1.3% in the US.36 Although its prevalence was only 0.84% in the current study, crustaceans were ranked at the second most common food allergen, indicating that shrimp and crab are important food allergens in Korean children.
A meta-analysis of 10 studies on anaphylaxis showed an incidence of 4.93 per 100 person-years in children aged 0-19 years.37 In our study, the overall prevalence of food-induced anaphylaxis in Korean schoolchildren was 0.97%. This high prevalence might be because we used a broad definition of anaphylaxis that reflects its potential severity, even if the actual reaction is not always life-threatening.18 Another reason for the high prevalence of food-induced anaphylaxis in the present study might be because we could not confirm the natural regression in this questionnaire survey. If a child never again ate the offending food after the anaphylactic reaction occurred, he or she was still regarded as having current food-induced anaphylaxis, leading to an overestimation of the prevalence. In the present study, we demonstrated that peanut, cow's milk, buckwheat, and hen's egg were commonly responsible for food-induced anaphylaxis. Among the food groups, fruits, crustaceans, tree nuts, and fish were frequent causes of anaphylaxis. Our results about major causes were similar to those in other studies. 383940 Of interest, buckwheat is an important causative food of anaphylaxis in Korea as well as in Japan.14 In contrast, anaphylaxis triggered by fruit ingestion might be overestimated, because mild subjective symptoms were included in determining the diagnosis of anaphylaxis.18
In conclusion, the prevalence of current immediate-type FA and food-induced anaphylaxis in Korean schoolchildren in 2015 was 4.06% and 0.97%, respectively. Peanut, cow's milk, hen's egg, fruits, crustaceans, and tree nuts are common allergens.





 XML Download
XML Download