

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mycoplasma pneumoniae is an important cause of community-acquired pneumonia (CAP) in children and young adults. Although M. pneumoniae often causes mild to moderate pneumonia, it can also be associated with more serious, life-threatening disease and a wide array of extrapulmonary manifestations.12
M. pneumoniae causes up to 40% or more of CAP cases, and as many as 18% of cases requiring hospitalizations in children.3
M. pneumoniae is innately resistant to all beta-lactams and glycopeptides due to the lack of a cell wall. In contrast, M. pneumoniae is susceptible to antibiotics that interfere with protein or DNA synthesis, such as macrolides, tetracyclines, and quinolones. During the last decade, macrolide-resistant M. pneumoniae (MRMP) has been reported worldwide, and its prevalence has generally increased.4 The prevalence of MRMP is especially high in East Asian countries, such as China, Japan, and Korea.456
Although the clinical course of MRMP pneumonia appears to be prolonged compared with macrolide-susceptible M. pneumoniae (MSMP) pneumonia,78 the clinical relevance of the increased prevalence of MRMP has not been definitely established. Therefore, continuous surveillance of the change in prevalence of MRMP pneumonia and the influence of MRMP on disease outcome are inevitably needed to define its clinical relevance and to develop appropriate treatment strategies at a time when MRMP is increasingly being detected.
M. pneumoniae infections occur both endemically and epidemically, in 3-7 years intervals for the latter. In Korea, M. pneumoniae epidemics have been observed in 3- to 4-year cycles since the mid-1980s.9 During the last several M. pneumoniae epidemics in Korea, the macrolide resistance rate has increased from 2.9% in 2003 to 62.9% in 2011.6 However, studies demonstrating changes in the clinical course of disease and in treatment strategies for M. pneumoniae pneumonia since 2011 are limited.
The aim of this study was to investigate the change in macrolide resistance rate in pediatric M. pneumoniae pneumonia and to evaluate the influence of MRMP on the clinical course of disease by comparing clinical characteristics of M. pneumoniae pneumonia that occurred during the epidemics of 2011 and 2015 in Korea.
MATERIALS AND METHODS
Study population
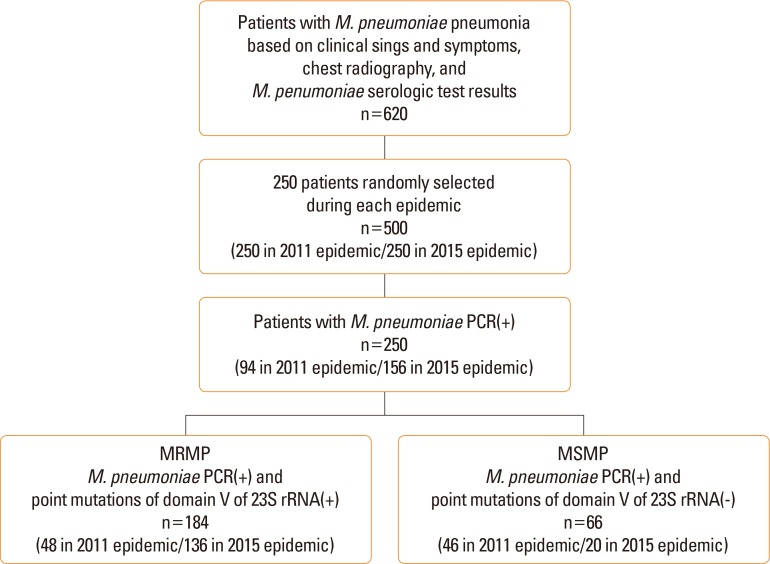
A retrospective cross-sectional study was carried out on pediatric patients with M. pneumoniae pneumonia admitted to Korea University Guro Hospital between August and December of 2011 and the same time frame in 2015. Among 620 patients diagnosed with M. pneumoniae pneumonia based on clinical symptoms, signs of lower respiratory tract infection, chest radiography, and serologic tests for M. pneumoniae (either microparticle agglutination assay titer of ≥1:160 or positive specific immunoglobulin M (IgM) against M. pneumoniae),10 250 patients were randomly selected during each epidemic. Among those patients, 94 patients in 2011 epidemic and 156 patients in 2015 epidemic were M. pneumoniae polymerase chain reaction (PCR) positive. These patients were divided into the MRMP and MSMP pneumonia groups based on the presence of specific point mutations in domain V of the M. pneumoniae 23S rRNA genes from nasopharyngeal aspirates (Figure).
The medical records of enrolled patients were reviewed retrospectively. Defervescence was defined as a body temperature below 38℃ for at least 24 hours without any use of antipyretics. Patients with pre-existing underlying diseases (such as congenital heart disease, bronchopulmonary dysplasia, immunodeficiency, or malignancy) were excluded. This study was approved by the Institutional Review Board of Korea University Guro Hospital.
Specimens and identification of MRMP
All blood samples and nasopharyngeal aspirates were obtained at the time of admission. Nasopharyngeal aspirates were stored at −80℃ until they were used for PCR assay at the end of each epidemic. M. pneumoniae DNA was detected by conventional PCR targeting a conserved part of the P1 adhesin gene.11 The point mutations at sites 2063 and 2064 in domain V of 23S rRNA genes were examined using a direct sequencing method as previously reported.12
Statistical analysis
All data are expressed as means and standard deviations, unless otherwise indicated. Continuous variables were compared with Student t or the Mann-Whitney tests. Differences in categorical variables were assessed with the χ2 test or Fisher's exact test. SigmaPlot software (Systat Software Inc., San Jose, CA, USA) was used for statistical analysis, and P values <0.05 were considered statistically significant.
RESULTS
Change in the macrolide resistance rate in M. pneumoniae pneumonia over 2 consecutive epidemics
Among 250 patients with positive M. pneumoniae PCR results, the resistant strain was detected in 51.1% (48/94) in the 2011 epidemic and 87.2% (136/156) in the 2015 epidemic. All MRMP isolates had the A2063G point mutation.
Changes in the clinical characteristics of M. pneumoniae pneumonia over 2 consecutive epidemics
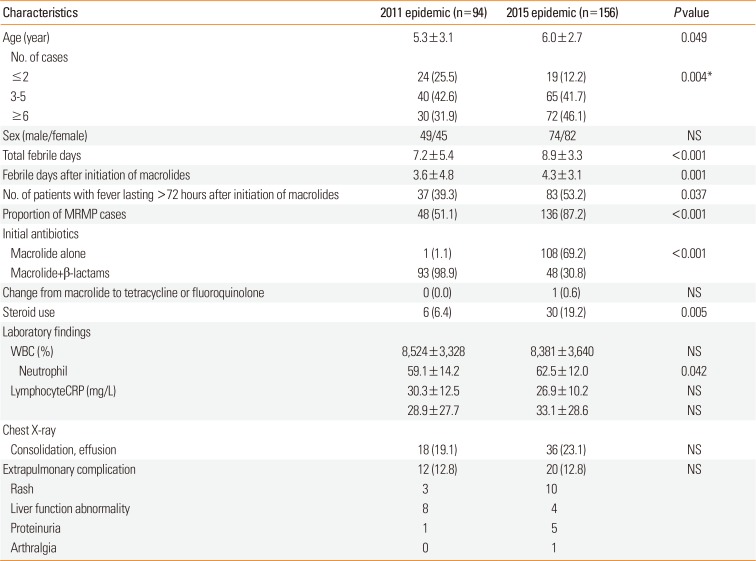
The clinical course and laboratory findings of patients with M. pneumoniae pneumonia in each epidemic are summarized in Table 1. Compared with the 2011 epidemic, the mean age of patients was increased, and both the total febrile days and the febrile days after initiation of macrolides were prolonged in the 2015 epidemic. The proportion of patients who had a fever lasting more than 72 hours after initiation of macrolides and who received corticosteroid treatment were also higher in the 2015 epidemic. However, chest radiologic findings and the incidence of extrapulmonary complications were not significantly different between the 2 epidemics. Among laboratory findings, the total white blood cell (WBC) count was not different between the 2 epidemics, though the relative proportion of neutrophils was higher in the 2015 epidemic.
Comparison of the clinical characteristics of MSMP or MRMP pneumonia between the 2 epidemics
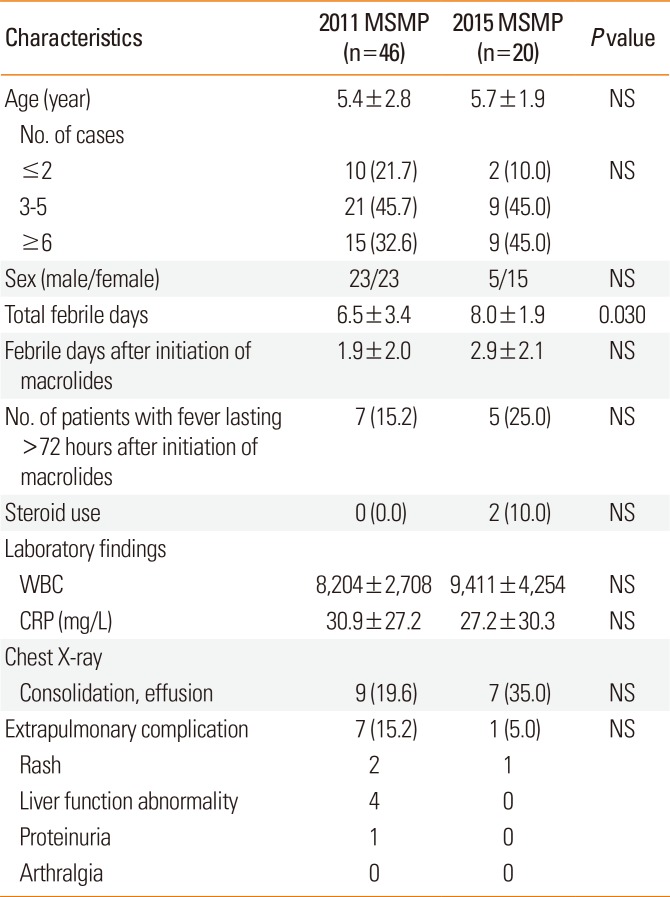
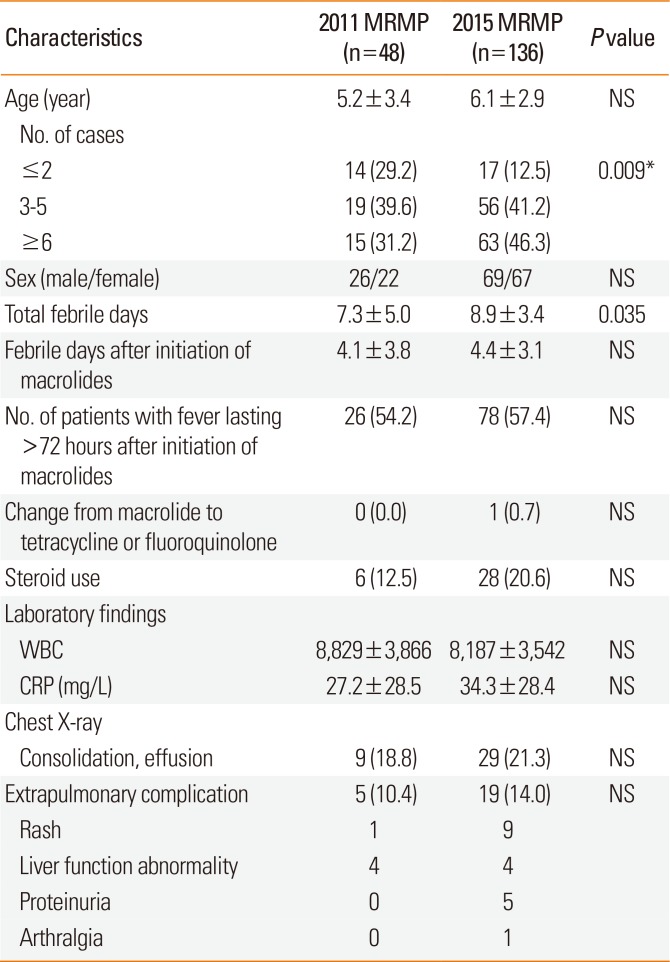
The clinical course and laboratory findings of patients with MSMP or MRMP pneumonia in each epidemic are summarized in Tables 2 and 3. Febrile days after initiation of macrolides, proportion of patients with a fever lasting more than 72 hours after initiation of macrolides, chest radiologic findings, and the incidence of extrapulmonary complications were not significantly different between the 2 epidemics in both groups. However, compared with the 2011 epidemic, total febrile days were prolonged in both groups, and number of patients with MRMP pneumonia increased significantly as the age increased in the 2015 epidemic.
Comparison of the clinical characteristics of MSMP and MRMP pneumonia during 2 epidemics
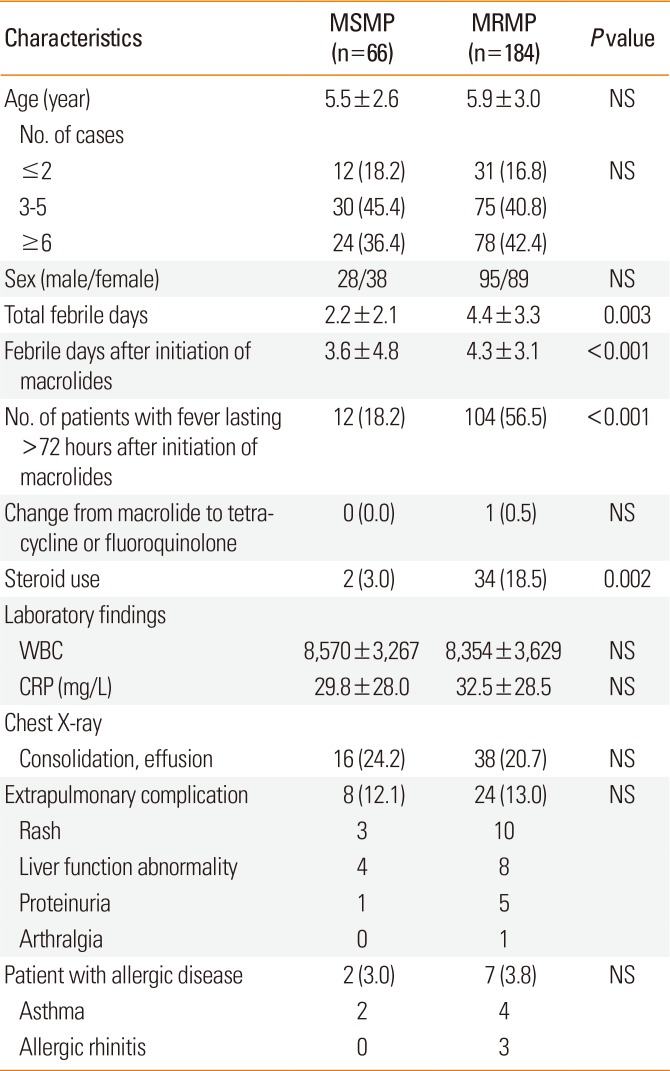
The clinical course and laboratory findings of patients with MSMP or MRMP pneumonia during the 2 epidemics are summarized in Table 4. Demographic data were not significantly different between the 2 groups. However, compared with patients with MSMP pneumonia, patients with MRMP pneumonia showed longer total febrile days and longer febrile days after initiation of macrolides. Both the proportion of patients with fever lasting more than 72 hours after initiation of macrolides, and the proportion of patients with corticosteroid use were higher in patients with MRMP pneumonia. Chest radiologic findings and the incidence of extrapulmonary complications were not significantly different between the 2 groups. The proportion of patients with asthma or allergic rhinitis was also not significantly different between the 2 groups.
DISCUSSION
In this study, we found that the macrolide resistance rate of M. pneumoniae rose from 51.1% in 2011 to 87.2% in 2015. In comparison of 2 epidemics, the mean age of patients with M. pneumoniae pneumonia was increased, and the total febrile days and febrile days after initiation of macrolides were prolonged in the 2015 epidemic. The overall severity of MRMP or MSMP pneumonia over 2 epidemics was not significantly changed. However, the proportion of patients who had a fever lasting more than 72 hours after initiation of macrolides and who received corticosteroid treatment were higher in MRMP pneumonia during 2 epidemics.
Macrolide resistance is mainly due to transition mutations at positions A2063 or A2064 in domain V of the 23S rRNA gene, a binding site of macrolide antibiotics.13 Based on previous studies to confirm that point mutations at the sites resulted in macrolide resistance, detection of these point mutations have been used as a marker for macrolide resistance.41415 An A-G transition at A2063 or A2064 confers a high level of resistance to macrolides. The A2063G transition is the most common mutation, followed by the A2064G transition.4 Although mutations at position A2067 and/or C2617 in domain V of the 23S rRNA gene are also associated with macrolide resistance, these mutations have rarely been reported. All MRMP isolates in this study had the A2063G point mutation in both epidemics, which is consistent with those of previous reports.
In Korea, the macrolide resistance rate of M. pneumoniae was 51.6%-62.9% in 2011.616 To our knowledge, there are no available data for the macrolide resistance rate since 2011. In the present study, the macrolide resistance rate in children with M. pneumoniae pneumonia was 87.2% in the 2015 epidemic, which is equivalent to that in China or Japan according to recent reports.1718 Considering the resistance rate was 51.1% in the 2011 epidemic, the macrolide resistance rate appears to be rising continuously and rapidly in Korea.
In this study, the mean age of patients with M. pneumoniae pneumonia was increased in the 2015 epidemic as compared with the 2011 epidemic. The change can be explained by increased proportion of MRMP pneumonia over the 2 epidemics because the peak age of MRMP pneumonia incidence was increased in the 2015 epidemic, in contrast to that of MSMP pneumonia incidence. This trend is different from those of recent M. pneumoniae epidemics in Korea. During the last several epidemics, the peak age of incidence appeared to be falling.19 However, there have been few studies to investigate the age distribution of patients with MRMP pneumonia. Thus, further studies are necessary to ascertain whether older age group is more susceptible to MRMP pneumonia as shown in the present study.
Although the prescription pattern of initial antibiotics was changed over 2 epidemics, this change was associated with change in the principles of empirical antimicrobial therapy in CAP at our hospital, but not associated with change in the severity of pneumonia at admission. Because there was limited information about the macrolide resistance rate of M. pneumoniae until the end of the 2011 epidemic in Korea, this affected the choice of initial antibiotics. Macrolide/β-lactam combination was used as initial antibiotics in most patients (93/94) in the 2011 epidemic, whereas macrolide monotherapy was used in most patients (108/156) in the 2015 epidemic, along with awareness that the main reason for prolonged clinical course in most patients has been the macrolide resistance, not co-infection with other bacteria. However, macrolide/β-lactam combination was prescribed to all patients with consolidation or effusion on chest radiography in both epidemics.
Information about the influence of macrolide resistance on clinical outcomes is critical to determining whether there is a need to change current treatment recommendations for pediatric M. pneumoniae pneumonia. Although previous data from patients with MRMP pneumonia suggest that the presence of resistance did not increase the overall severity of disease, recent reports have demonstrated that disease progression during therapy, with increased complications, occurred in patients with MRMP pneumonia.2021 Surveillance data from Japan have also shown that cases requiring hospitalization have gradually increased as MRMP pneumonia in children increased.8 The reason for the difference in the influence of MRMP on clinical outcomes in previous studies could be partially explained by the fact that patients with MRMP pneumonia had more persistent signs and symptoms, which in turn led physicians to add an adjunctive treatment, such as corticosteroids, or to replace antibiotics in order to obtain a more rapid clinical improvement. In the present study, although the overall severity, including extrapulmonary complications between MSMP and MRMP pneumonia, was similar (except for the prolonged clinical course), the proportion of patients who received corticosteroid treatment was also higher in patients with MRMP pneumonia than in those with MSMP pneumonia. Because we used corticosteroids for cases with rapid progression despite the initiation of macrolides or cases with high fever lasting more than 5 days regardless of the macrolide resistance state, the higher proportion of corticosteroid use in MRMP pneumonia cases may reflect a higher disease severity in this group.
A previous study demonstrated that atopic sensitization and history of asthma were associated with macrolide treatment failure in patients with M. pneumoniae pneumonia.22 However, there is no study to investigate whether patients with allergic disease are more susceptible to MRMP infection. In the present study, there was no significant difference in the proportion of patients with allergic disease between the MSMP and MRMP pneumonia groups. Therefore, macrolide treatment failure in the patients with asthma does not seem to be associated with MRMP infection. However, because the numbers of patients with allergic disease in those studies were relatively small, further studies are necessary to confirm the results and to elucidate underlying mechanisms for macrolide treatment failure in M. pneumoniae pneumonia patients who have asthma.
The adjunctive use of corticosteroids is based on previous studies suggesting that the host immune response plays a role in severe M. pneumoniae pneumonia.232425 In the current study, this therapeutic approach did result in rapid clinical improvements and resolution of pulmonary lesions associated with M. pneumoniae pneumonia, consistent with previous studies. Only 1 patient showed disease progression despite steroid use, and this patient also showed clinical improvement after switching from macrolide to fluoroquinolone antibiotics. Considering possible adverse effects, there is a need to more clearly define indications for corticosteroid use and to use alternative antibiotics with caution until new antibiotics that are safe and effective against MRMP in children are available.
One interesting result from this study is that patients with MSMP pneumonia showed increased total febrile days and a weak trend of increased febrile days after initiation of macrolides, over the 2 consecutive epidemics. One explanation for this result is the possible acquisition of resistance to macrolides during treatment. In fact, several recent in vitro and in vivo studies have demonstrated that M. pneumoniae acquires macrolide resistance within a few days of administration of macrolide antibiotics.262728 However, we could not confirm this due to a lack of samples which were collected at different time points during the treatment course. Therefore, to properly evaluate the influence of MRMP on clinical outcomes, re-testing of the macrolide resistance state during treatment based on the individual clinical situation should be done in future studies.
The inclusion of patients from 2 recent, consecutive epidemics and a relatively large sample size are the strengths of this study. However, there were some limitations in this study, including its retrospective design. First, not all children with M. pneumoniae pneumonia were included because we enrolled only moderate to severe PCR-positive patient who needed hospitalization. Although some previous studies included outpatients, those did not present data about the macrolide resistance rate in outpatients separately, which makes it difficult to estimate the resistance rate in mild cases. Therefore, future studies are still necessary to investigate the difference in the resistance rate between mild and moderate-to-severe cases. Secondly, other mutations associated with macrolide resistance were not searched because resistance to macrolides in East Asia has been mainly due to A2064G and A2064G, and thus there is a possibility that the resistance rate may be underestimated. Thirdly, all patients were from a single tertiary hospital and thus do not represent the general pediatric population in Korea. However, the macrolide resistance rates in this study sufficiently suggest that the prevalence of MRMP is rising rapidly in Korea because the resistance rate was measured in the same tertiary hospital over 2 consecutive epidemics.
In conclusion, the macrolide resistance rate of M. pneumoniae has risen rapidly over 2 recent, consecutive epidemics, and this was associated with a prolonged clinical course of disease in pediatric M. pneumoniae pneumonia. The relative proportion of patients receiving corticosteroids as an adjunctive therapy was significantly higher in cases of MRMP pneumonia during both epidemics, suggesting that the severity of MRMP pneumonia may be higher than that of MSMP pneumonia. Large-scale surveillance studies including outpatients with mild disease are needed to investigate the prevalence of MRMP pneumonia and its true impact on clinical outcomes in Korean children.
 XML Download
XML Download