

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anaphylactic response to drugs manifests as a respiratory distress due to laryngeal edema and intense bronchospasm, often followed by vascular collapse or shock.1 Several redisposing factors are associated with hypersensitivity reactions to drugs in patients. Antibiotics, anesthetics agents, non-steroidal anti-inflammatory drugs, and opiates are common triggers of anaphylaxis.2
Severe hypersensitivity reaction during general anesthesia is one of the most frequent drug-induced anaphylactic reactions, as recently shown by several studies in the United States.3 Diagnosis of perioperative anaphylaxis is complicated as the patient is often sedated and thus unable to alert the physician of symptoms. Additionally, diagnosis can be hampered by obstruction of skin manifestations with surgical drapes, and cardiac events associated with anaphylaxis can be mistaken for other causes of cardiovascular collapse. Furthermore, multiple drugs are frequently administered simultaneously or in rapid succession during surgery. Most hypersensitivity reactions occur within minutes after administration of the drug; however, depending on the agent and time of administration, reactions can be late-onset.4 Common drugs causing anaphylaxis include neuromuscular blocking agents, latex, antibiotics, hypnotics, opioids, and colloids.
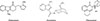
Palonosetron is a 5-hydroxytryptamine3 (5-HT3) antagonist used for the prevention and treatment of nausea and vomiting due to cancer chemotherapy and surgery. Other commonly used 5-HT3 antagonists include ondansetron and granisetron (Fig. 1). Additionally, ondansetron- and granisetron-related hypersensitivity reactions have been reported in 8 and 2 patients, respectively.5,6,7,8,9,10
In this report, we describe a patient who developed anaphylaxis during general anesthesia following intravenous palonosetron administration.
CASE REPORT
A 37-year-old male was admitted for kidney donation. Prior to surgery, he underwent the following tests for routine evaluation: dimercaptosuccinic acid (DMSA) renal scan, pulmonary function test, abdominopelvic computed tomography, and echocardiogram. His left atrium was mildly enlarged (42 mm), as seen from the echocardiogram; however, no other abnormalities were found. Serological tests showed that the patient was negative for cytomegalovirus, human immunodeficiency virus, hepatitis C virus, and hepatitis B virus.
As shown in Fig. 2, for general anesthesia, rocuronium, fentanyl, and sodium pentothal were administered for intubation, and desflurane was used for maintenance. The surgery was uneventful until administration of palonosetron at 2 hours 20 minutes after the start of the surgery. Five minutes later, the patient's blood pressure (BP) decreased from 140/90 at baseline to 80/50 mm Hg, his heart rate increased from 65 to 80 per minutes, and his oxygen saturation was 98%. During resuscitation, 5 mg of ephedrine was administered twice, but no response was achieved; thus, 10 mg of ephedrine was administered 2 more times. Thirty minutes after palonosetron administration, the patient developed facial and lip edema, conjunctival swelling, and rashes on the face and chest. Thus, 100 mg of hydrocortisone and 4 mg of chlorpheniramine were intravenously administered for treating the rash. Physical examination performed at that time revealed generalized wheezing over both lungs. Therefore, a salbutamol nebulizer (Ventolin) was administered. The results of laboratory tests conducted for differential diagnosis were as follows: blood glucose, 156 mg/dL; sodium, 137 mmol/L; potassium, 3.6 mmol/L; chloride, 105 mmol/L; lactate, 2.2 mmol/L; and hemoglobin, 13.6 g/dL. Thus, bleeding and hypovolemia were excluded from the differential diagnosis. No other intraoperative complications were found.
After the surgery, the patient was admitted to the intensive care unit for close monitoring, and delayed anaphylaxis was not observed. No further reaction was reported over the following 72 hours. Serum tryptase levels measured 3 hours and 1 day after anaphylaxis were 8.60 and 1.20 µg/L, respectively.
The patient had no prior history of allergies to drugs/food or history of allergic dermatitis, rhinitis, or asthma. He had undergone herniorrhaphy eight years ago, with no adverse events. However, given the severity of the hypersensitivity reaction, a skin test was performed to evaluate the patient's response to palonosetron on days 1, 17, and 54 following the surgery. The skin test was negative on days 1 and 17, but was positive at 1:100 dilution of the allergen (0.5 µg/mL) on day 54 (Fig. 3).
DISCUSSION
Palonosetron is a second-generation 5-HT3 receptor antagonist used for postoperative nausea and vomiting (PONV). Palonosetron is superior to ondansetron and granisetron for PONV prophylaxis due to prolonged duration and minimal side effects.11 The most common adverse effects of palonosetron in PONV are QT prolongation, bradycardia, headache, and constipation.12
This is the first report of a patient who developed anaphylaxis to palonosetron in Korea. While 1 or more of the anesthetics used in the perioperative period, namely rocuronium, sodium pentothal, and fentanyl, could potentially cause anaphylaxis, they were unlikely to cause serious conditions. Anaphylaxis is an immediate reaction, and patient's symptoms, starting with hypotension, emerged 2 hours after anesthesia induction, within a few minutes after palonosetron injection. The incidence of anaphylaxis to palonosetron is low; however, there was a strong correlation between the time after palonosetron administration and the symptoms. Thus, the patient was diagnosed with anaphylactic reactions to palonosetron.
Review of the literature revealed 2 previous case reports of anaphylactic reactions to palonosetron. One case involved a 40-year-old female who developed hypotension and hypoxia within minutes following palonosetron administration.7 The second case was of a 40-year-old female patient who developed hypotension and bradycardia, and was resuscitated with fluid and diphenhydramine.9 No other cases with definitive anaphylaxis diagnosis were reported.
Palonosetron is a relatively new drug with unexpected side effects reported in a post-marketing survey.12 The other relatively well-known 5-HT3 antagonist, ondansetron, was also reported to have an association with hypersensitivity.6,7,8,9,10 Two patients who developed anaphylaxis following ondansetron administration were assessed by using an intradermal test, which was positive at ondansetron doses of 0.02 and 0.002 mg/mL, respectively. Intriguingly, the skin prick test was negative in both patients.
In recent reports, a patient who experienced ondansetron-related hypersensitivity had no reaction to granisetron or palonosetron.5,8 Ondansetron, granisetron, and palonosetron do not share a common indole ring, which might be one of the reasons for the lack of cross-reactivity between these 5-HT3 antagonists.
In summary, as illustrated in this case of intraoperative anaphylaxis, albeit rare, palonosetron should be considered as a cause of anaphylaxis.


 XML Download
XML Download