

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a chronic inflammatory airway disease characterized by bronchial hyper-responsiveness and reversible airway obstruction.1 Chronic inflammation of the airways causes proliferation of smooth muscle cells and fibroblasts that eventually lead to dysplasia of the alveolar epithelial cells. If not treated, these changes can lead to irreversible airway remodeling that progressively worsens pulmonary function.2 Even well-controlled, asymptomatic asthma can be exacerbated by bacterial or viral infections, stress, or exposure to allergens.
Inhaled corticosteroids (ICSs), a current mainstay asthmatic maintenance drug, effectively inhibits inflammatory airway reactions and prevents asthma exacerbation. Long-term management treatment with ICSs may impede the progressive decline of lung function and irreversible airway remodeling.2,3 Global Initiative for Asthma (GINA) guidelines recommend long-term maintenance treatment with ICSs even for patients with 'well-controlled' mild persistent asthma.1 However, in clinical practice many asthmatics voluntarily discontinue their maintenance teratment against the recommendations of physicians.4
We surveyed asthma outpatients lost to follow-up within 3 years after initial diagnosis to investigate the factors that affected non-adherence to asthmatic management and to determine the impact of discontinued asthma maintenance treatment on the clinical course of their asthma.
MATERIALS AND METHODS
Study population
The study population consisted of 475 adult patients newly diagnosed with asthma at the Allergy Clinic of Seoul National University Hospital between January 2005 and March 2007. A diagnosis of asthma was made by measuring an increase of at least 12% and 200 mL of the forced expiratory volume in 1 second (FEV1) from the baseline level at 15 min after the administration of salbutamol or a positive methacholine bronchial provocation test where the provocative concentration causing a 20% fall in FEV1 (PC20) was lower than 16 mg/mL.
Study method
A retrospective review of electronic medical records was conducted to identify if patients had continued to follow-up in the initial 3 years since they were diagnosed with asthma. Lost to follow-up patients for at least consecutive 7 months were defined as non-adherent; the follow-up duration was the time ininterval of the first and last visit. Patients who had continued to follow-up at least 3 years were defined as adherent (Fig. 1).
Using electronic medical records, we investigated the following: the baseline characteristics of patients; the presence of atopic dermatitis, allergic rhinitis and chronic sinusitis; pulmonary function tests including FEV1 and forced vital capacity (FVC); PC20; eosinophil percent in induced sputum; and the existence of respiratory symptoms.
A telephone survey was conducted on patients who were lost to follow-up. We investigated the reasons for non-adherence, whether they were receiving management treatment for asthma at other facilities, and if they had experienced episodes of acute exacerbation or hospital admission. In addition, we asked for the score of the Asthma Control Test (ACT) and the presence of chronic cough which is a component of the Korean ACT (K-ACT) to assess current symptoms and asthma control status.5
Statistical analysis
Statistical analysis was performed using SPSS version 17.0. Descriptive statistics are shown as the mean±standard deviation (SD). Chi-square tests and Fisher's exact tests were conducted to assess the statistical association between the continuation of hospital visits and nominal variables; in addition, a Student's t-test and Mann-Whitney test assessed any association with categorical variables. A Kaplan-Meier survival analysis further investigated the effect of the associated variables on the continuation of management treatment. Odds ratio (OR) and 95% confidence interval (CI) were calculated with binary logistic regression and Cox regression to adjust for various factors that could influence the study outcome. A P value of less than 0.05 was defined as statistically significant.
RESULTS
Clinical characteristics of patients
A total of 475 adult patients were newly diagnosed with asthma between January 2005 and March 2007. The age of the study subjects ranged from 14 to 92 years (mean±SD, 51.0±17.9 years). Initial pulmonary function tests showed that the mean FEV1 and FVC value were 85.3% and 94.0%, respectively; in addition, the mean methacholine PC20 was 6.2 mg/mL. Sputum eosinophilia was observed in 311 of 462 patients (67.3%) and the mean sputum eosinophil percentage was 10.5%. Based on a skin prick test, 153 of 386 patients (39.6%) had atopic traits. Lower respiratory symptoms (such as cough, sputum, or wheezing) were observed in 300 of 397 patients (75.6%) and 182 of 350 patients (52.0%) had sinusitis on the paranasal sinus radiography. Table 1 summarizes all other characteristics of the study participants.
A total of 402 patients (84.7%) were prescribed ICSs after confirming the presence of asthma; treatment included ICSs only and ICSs combined with long acting β2-agonist (LABA). A leukotriene receptor antagonist (LTRA) was prescribed in 246 patients (51.8%). One hundred and eight patients (22.7%) used oral or systemic steroids at least once during the follow-up period.
Comparison of the patients in relation to adherence to the clinical follow-up investigation
A total of 351 patients (73.9%) were lost to follow-up within 3 years after the diagnosis of asthma. Compared to the continued follow-up group, the loss to follow-up group had higher FEV1 and PC20 values (P<0.05) and tended to be younger (P<0.05). The rate of ICSs monotherapy was higher while the rate of LTRA use was lower in the loss to follow-up group compared with the continued follow-up group.
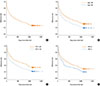
A Kaplan-Meier survival analysis and Cox regression showed that variables like age ≥50 years, FEV1 <80%, presence of lower respiratory symptoms; in addition, the use of a LABA and ICSs combination or LTRA were associated with longer adherence to asthma treatment (Fig. 2).
The causes of non-adherence and clinical progression in the loss to follow-up group
Among the 351 patients who had discontinued follow-up treatment, 196 patients (55.8%) responded to the telephone survey. The mean time interval from last outpatient clinic visit to the telephone survey was 1,551.6±402.4 days. Table 2 and Fig. 3 shows that the most common reason for lost to follow-up was the improvement in asthma symptoms (59.5%). The sec most common reason was the travel inconvenience due to long distance to the hospital (18.4%). Other causes of loss to follow-up were: long waiting times (5.4%), no improvement (3.8%), cost (1.6%), a physician's recommendation (1.5%) and others (9.7%). Seventy-two responders (36.7%) continued asthma treatment at other medical facilities; however 124 responders (63.3%) had not been adhered to asthma treatment since they discontinued follow-up.
On the question asking the current control status, 133 responders (67.8%) answered that their asthma symptoms had improved and were maintained in a well-controlled status and 58 responders (29.6%) replied that the degree of their asthma symptoms were similar compared to when they actively received asthma treatment. Only 1 patient (0.5%) answered that his asthma was aggravated.
Comparison of patients who were lost to follow-up according to treatment continuity
The survey responders of the loss to follow-up group were categorized according to if they were or were not continuing asthma management at other facilities (ongoing treatment group versus non-treatment group). Table 2 shows that patients belonging to the non-treatment group (compared to the ongoing treatment group) were younger (P<0.001) and had higher initial FEV1, FVC, and PC20 values (P=0.049, P=0.018 and P=0.039, respectively). However, there were no significant statistical differences in the sputum eosinophil and neutrophil proportion between these two groups (P=0.248 and P=0.213, respectively).
Thirty-one of 63 patients (49.2%) in the ongoing treatment group responded that they stopped follow-up because of travel inconvenience to the hospital while 80.3% of the non-treatment group discontinued follow-up because their asthma symptoms had improved. In the ongoing treatment group, episodes of acute asthma exacerbation were observed in 6 patients (4.8%), and only 1 patient (0.8%) experienced hospitalization. However, there were no significant differences compared to the non-treatment group (4.5%, P>0.05 and 0%, P>0.05, respectively).
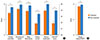
Ninety-six patients in the non-treatment group (77.4%) answered that their asthma symptoms had improved despite discontinued management treatment. The current mean total ACT score and cough score (for K-ACT) in these patients were significantly higher than that of the ongoing treatment group (P<0.001 and P=0.026, respectively) (Fig. 4).
DISCUSSION
Asthma is a common chronic disease and around 400 million people in the world have asthma; in addition, there may be an additional 100 million asthma cases by 2025 due to increased trends in the diagnosis of asthma.1,6 The estimated cost of asthma in the United States was $12 billion in 1994; subsequently, it has increased to $56 billion in 2007.7 The cost related to asthma in the Republic of Korea was about $4 billion in 2004; in addition, it has also recently increased.8 According to the data from National Health Insurance Corporation (NHIC) in Korea, payments for outpatient services and medical prescriptions accounted for 83% of the direct costs for asthma.8 Efforts to reduce costs associated with asthma are necessary due to the immense public health and economic burden.
ICSs effectively improve asthma symptoms and lung function as well as decrease the likelihood of developing episodes of acute exacerbation.3 GINA guidelines recommended the maintenance of ICSs in moderate and persistent asthma as well as in well-controlled mild asthma.1 However, adherence to management treatment in asthma patients ranged from less than 30% to 70%9,10 and half of the patients did not maintain ICSs contrary to the recommendation of a physician.11
There is continued controversy over the long-term efficacy of maintenance treatment with ICSs. The long-term outcome of ICSs with anti-inflammatory effects is not prominent in mild persistent asthma compared to moderate or severe asthma.12-14 In recent childhood asthma studies, airway remodeling might arise from the acute exacerbation of asthma and not chronic inflammation.15 ICSs could inhibit the chronic inflammation of the airways; however, it did not change the airway remodeling and the subsequent progressive decline of lung function or long-term prognosis.16,17
According to GINA guidelines, maintenance treatment can be discontinued if patients have not experienced asthma symptoms for at least 1 year while using the lowest dose of ICSs.1 However, the appropriate ICSs management duration for asthma patients with well-controlled mild or moderate symptoms is unclear. Therefore, an investigation of the clinical course and long-term prognosis of patients who had discontinued asthma management treatment will be helpful to understand the natural course of asthma after discontinued ICSs management.
In our study, 50% of adult asthma patients discontinued outpatient clinic visits within 1 year and only 25% of the patients maintained follow-up for 3 years. Telephone surveys indicated that only 1.5% of the responders who stopped visiting outpatient clinics had discontinued asthma management treatment based on the recommendation of a physician while most of the responders voluntarily discontinued medical follow-up regardless of the medical necessity for management treatment. The main indicated cause of non-adherence was the symptoms improvement. Most responders (90%) who had discontinued follow-up due to travel inconvenience had maintained treatment for asthma at other facilities while most of the responders who had discontinued follow-up due to symptom improvement did not take any asthma medication.
Discontinued ICSs treatment does not always cause aggravation in clinical parameters such as subjective asthma symptoms or number of acute exacerbations for mild to moderate asthma.18,19 The frequency of acute exacerbations or admissions was not significantly different in mild asthma patients who used inhaled or oral corticosteroids only when acute exacerbations occurred compared to patients who continuously maintained ICSs.14 In our study, asthma was controlled asymptomatically in most non-adherent patients that did not receive asthma management treatment and only a few non-adherent patients experienced episodes of acute exacerbations over the course of 3 years.
Long-term ICSs use is associated with adverse effects such as oral candidiasis,20 cataracts,21 bone loss,22 and growth retardation in children;23 subsequently, the discontinuation of unnecessary management treatment can prevent adverse effects. Considering the low treatment adherence rate and the uncertain preventive effects on airway remodeling, management treatment with ICSs may not be practical in current clinical practices for patients with mild asthma. Acute asthma exacerbation related to the discontinuation of ICSs might be prevented though the treatment of mild persistent asthma with short and intermittent courses of inhaled or oral corticosteroids administered when symptoms exacerbate.14 The risk of developing acute exacerbations can be predicted by measuring the eosinophil count in induced sputum after discontinuation of the ICSs management treatment.24
Further studies are required to help predict asthma relapse in asymptomatic patients without management treatment and early-stage treatment of the disease. Subsequently, optimized and personalized asthma treatment can be developed according to the inflammation status of individuals. Up to 20% of the economic costs of asthma are associated with treating mild asthma; therefore, social and economic burdens can be reduced by discontinued mild asthma treatment for patients who do not need ICSs management.




 XML Download
XML Download