

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dietary sugar is an increasingly critical public health concern worldwide, as a high dietary intake of sugar, particularly added sugars or free sugars, is associated with an increased risk of chronic diseases such as obesity, type II diabetes, hypertension, and metabolic syndrome [1234]. Thus, the World Health Organization (WHO) strongly recommends a reduction in free sugar intake to < 10% of total energy intake [5].
Total sugar intake is the sum intake of all free mono- and disaccharides. Total sugars can be categorized based on their source into naturally occurring sugars such as fruits and milk as well as added sugars such as processed foods [6]. Various types of dietary sugars have different nutritional values. Major food sources of added sugars are soft drinks, cakes, candies, ice cream, and so on [7891011], which are high-calorie but low-micronutrient foods. In contrast, foods that contain naturally occurring sugars also have other essential nutrients, including vitamins and minerals. Louie and Tapsell [12] reported that added sugar is a more reliable indicator of poor diet quality and nutrient dilution than total sugar. Most studies involving adolescents in other countries also focused on added sugar intake or consumption of sugar-sweetened beverages (SSBs). A study in Brazil reported that 12.3% of energy was obtained from added sugar intake, and the major source was soft drinks [13]. A study in Taiwan reported that high SSB consumption was associated with metabolic syndrome components among boys [14].
Despite the lack of a dietary sugar database in Korea, several studies have reported the dietary sugar intakes of Korean children and adolescents. However, these studies assessed dietary sugar intake using a limited food list from school meals [151617] and partial snacks [1819] or a 1-day dietary record [2021]. However, Lee and colleagues recently established a database of total sugars for Korean food items and reported that dietary sugar od items for total sugar intake intake was highest in adolescents [22].
In exploring the relationship between dietary sugar intake and chronic disease, it is important to examine not only dietary sugar intake as well as relevant food sources but also their link to dietary behaviors and patterns. Dietary patterns are based on eating behaviors, and studying dietary patterns provides information on dietary practices [23]. Thus, investigating associations between dietary sugar intake and dietary patterns can be useful to establish an effective nutrition education program and policy for reducing dietary sugar intake.
Dietary behaviors during adolescence play an important role in determining long-term health [24]. Nevertheless, adolescents are likely to have poor dietary behaviors, for example, snacking, skipping meals, and eating out [25]. In addition, Song et al. [26] reported that the dietary patterns of Korean adolescents changed gradually from a traditional diet to Western diet between 1998 and 2005. According to the 11th Korea Youth Risk Behavior Web-based Survey, 37.5% and 28.3% of subjects consumed snacks and soft drinks, respectively, more than three times per week; moreover, the proportion of soft drink consumers has increased continuously over the last 5 years [27].
However, the relationship between dietary sugar intake and dietary behaviors in the Korean population has not been investigated to date. Therefore, this study aimed to estimate dietary sugar intake and relevant food sources according to sex, and to examine the relationship of dietary sugar intake with frequent snacking and dietary patterns among Korean children and adolescents using multiple-day dietary records.
SUBJECTS AND METHODS
Study subjects and design
We pooled data from five studies on Korean children and adolescents from 2002 to 2011 and conducted a secondary data analysis. The details of each study can be found elsewhere [2829303132], and an outline of the five studies can be found elsewhere [33]. In brief, all studies used the same protocol for dietary assessment (subjects completed at least 3 days of dietary records and had general demographics even though outcome varied by study). The study subjects were recruited from either schools or the pediatric center of a university hospital, and all had no known disease. Of the 4,088 eligible subjects, we excluded those with missing data for anthropometric measurements such as height and weight, maternal education, and physical activity. The final sample included 2,599 children and adolescents (1,048 boys and 1,551 girls) aged 9-14 years. The Institutional Review Board at Seoul National University approved this study, and informed consent was obtained from each participant (E1501/001-010).
Dietary assessment and dietary sugar intake
Dietary records were collected for 3-7 days, depending on the study; all subjects completed > 3 days of dietary records including one weekend day. All nutrient intakes were estimated using the Computer Aided Nutritional Analysis Program 3.0 (CAN-Pro; the Korean Nutrition Society) or DS24 (Seoul National University) software. Details of the dietary data have been described elsewhere [33].
Dietary sugar intake was estimated using a database of total sugars for Korean food items, which was recently developed by Lee et al. [22] and expanded in this study. This database includes only the total amount of sugar for each food item; therefore, we estimated total sugar intake from four major food sources (fruits, milk, processed foods, and commodity type foods) according to our previous study [33]. The food items included in each food source type are shown in Table 1.
Dietary patterns and snack intake
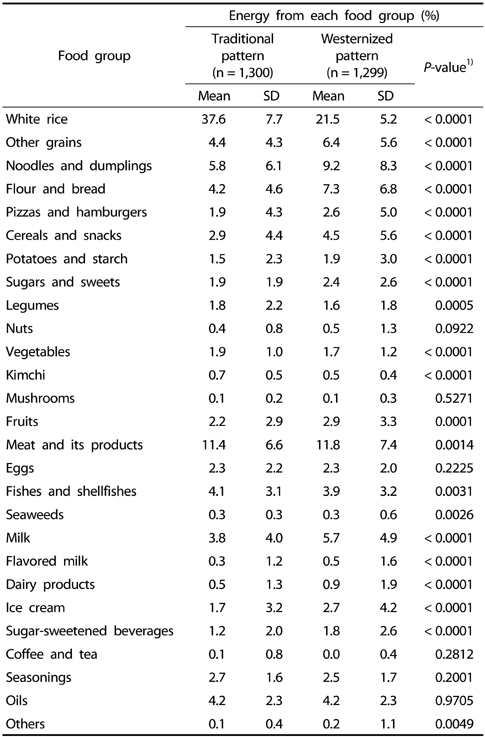
To identify dietary patterns, food items were categorized into 27 groups. Several food groups-such as grains, milk, and beverages-were subdivided according to foods commonly consumed by Korean children and adolescents to address actual dietary patterns. Grains, which are a staple food for Asians, were classified into the following six subgroups: white rice, other grains, noodles and dumplings, flour and bread, pizzas and hamburgers, and cereals and snacks. To differentiate snack patterns, milk and milk products were divided into milk, flavored milk, dairy products, and ice cream; and beverages were classified into SSBs and coffee/tea. SSBs refer to all types of sugar-sweetened beverages, including carbonated beverages, fruit and vegetable drinks, sport drinks, flavored soymilk, and sweetened tea and coffee drinks. Brewed coffee/tea and 100% fruit juice were separated from SSBs. The individual food amount was calculated as the percentage of total energy from each food group. K-mean cluster analysis was carried out using the percent energy obtained from each food group.
Two dietary patterns were derived by cluster analysis: Traditional and Westernized patterns. Table A1 presents the mean percent of energy from each food group in the two dietary patterns. The Traditional pattern was characterized by high consumption of white rice, legumes, vegetables, kimchi, and fishes, and shellfishes, which are typical foods in the traditional Korean diet. In contrast, the Westernized pattern was characterized by high consumption of noodles and dumplings, flour and bread, pizzas and hamburgers, cereals and snacks, sugars and sweets, fruits, milk, ice cream and frozen confections, and SSBs.
Since snacking is an important factor in dietary behavior, snack intake patterns and dietary sugar intake associated with frequent snacking were also examined. We defined snacks as all foods and drinks consumed at times other than during three regular meals (breakfast, lunch, and dinner). Subjects were divided into tertile groups according to energy intake from snacks by sex, and the dietary sugar intake for each tertile group was estimated.
Anthropometric data
Information on height and weight was obtained, and body mass index (BMI) was calculated based on height and weight (kg/m2). Weight status was determined using the national reference age- and sex- specific percentiles of BMI from the Korean Growth Chart (2007); i.e., 85th ≤ BMI < 95th percentile for overweight and BMI ≥ 95th percentile or BMI ≥ 25 kg/m2 for obesity. Subjects whose BMI percentiles were within the range of overweight but higher than 25 kg/m2 were defined as obese.
Confounding variables
Confounding variables included sociodemographic factors such as age, sex, and maternal education; physical activity was included as a lifestyle factor. Due to the use of different variables and categories in the five studies considered, we categorized confounding variables. Maternal education was classified as middle school or less, high school, and college or more. Regarding physical activity, subjects were defined as "physically active" if they performed moderate or vigorous physical activity for at least 20 min per day on three of the previous seven days [34]. In addition, the study number was used as a confounding variable to adjust for discrepancies among the five studies.
Statistical analyses
All statistical analyses were performed using the Statistical Analysis System (SAS version 9.3, SAS Institute, Cary, NC, US). All P-values were two-sided, and P < 0.05 was considered to indicate statistical significance. All analyses were stratified according to sex due to differences in physical development between boys and girls. Categorical variables were evaluated using the chi-square test, and continuous variables were assessed using a generalized linear model (GLM). Mean daily sugar and snack intake were estimated as adjusted mean ± standard error (SE) using the GLM. Dietary patterns were determined by cluster analysis in the PROC FASTCLUS procedure, and the significance of differences in the percent of energy intake from each food group between dietary patterns was tested using the GLM.
RESULTS
General characteristics of study subjects
The final study population comprised 2,599 Korean children and adolescents (1,048 boys and 1,551 girls). The general characteristics of study subjects according to sex are summarized in Table 2. The mean age of boys was 11.8 ± 1.7 years and that of girls was 11.1 ± 1.7 years. Boys tended to have higher height, weight, and BMI than girls (P < 0.0001 for all variables). Additionally, significantly more boys than girls were obese (13.9% of boys and 7.7% of girls) (P < 0.0001). The maternal education level was slightly higher in girls than in boys, but there was no significant difference. Boys (57.2%) were significantly more physically active than girls (43.8%; P < 0.0001).
Dietary sugar intake and its food sources
Mean daily sugar intakes according to food source are presented in Table 3. Total sugar intake was higher in girls (54.3 ± 0.8 g) than in boys (46.6 ± 0.9 g; P < 0.0001) after adjustment for confounding variables. Girls consumed 12.5% of their energy from total sugars compared to 10.8% for boys (P < 0.0001). Among food sources, processed foods made the greatest contribution to total sugar intake, followed by fruits and milk. Sugar intake from processed foods was 27.9 ± 0.7 g (6.4% of energy) for boys and 34.9 ± 0.6 g (7.9% of energy) for girls (P < 0.0001). Sugar intake from fruits was significantly greater in girls (8.8 g ± 0.4 g for girls and 7.5 ± 0.4 g for boys; P = 0.0081). However, intake of sugars from milk was slightly greater in boys, but there was no significant difference.
Processed foods were categorized into four subgroups. Sugar intake according to type of processed food in both sexes was examined (Fig. 1). The average sugar intake from processed foods was greatest for sweets such as candies and ice cream (13.3 ± 0.4 g), followed by beverages, flavored milk, and yogurt (8.6 ± 0.4 g), breads, snacks, and rice cakes (6.7 ± 0.3 g), and others (6.3 ± 0.2 g) in girls. This trend was also observed in boys. Girls consumed a 1.5-fold greater quantity of sugars from sweets such as candies and ice cream than boys (8.6 ± 0.4 g for boys and 13.3 ± 0.4 g for girls; P < 0.0001).
Frequent snacking and dietary sugar intake
Overall, 97.4% of subjects consumed snacks during the study period (data not shown). Snacks were consumed more frequently by girls than boys (Table 3). The mean daily number of snack foods was 3.9 ± 0.1 for boys and 5.2 ± 0.1 for girls (P < 0.0001), and the percent energy from snacks was higher in girls (25.0%) than in boys (21.2%; P < 0.0001).
Table 4 presents the dietary sugar intake across tertiles of energy intake from snack foods according to sex. After adjustment for confounding variables, total sugar intake showed a significantly increasing trend with energy intake from snack foods in both sexes (P < 0.0001 for both sexes). Sugar intake from food sources also increased with increasing energy intake from snack foods. Sugar intake from processed foods increased markedly with frequent snacking. Sugar intake from processed foods in the highest tertile was 46.3 ± 1.3 g for boys and 45.1 ± 1.0 g for girls, whereas that in the lowest tertile was 19.1 ± 1.3 g for boys and 22.1 ± 0.9 g for girls.
Dietary patterns and dietary sugar intake
Sugar intake differed significantly according to dietary pattern (Table 5). The mean daily total sugar intake of the Westernized pattern was 56.2 ± 1.3 g for boys and 57.2 ± 1.0 for girls, which was significantly higher than that of the Traditional pattern (46.5 ± 1.2 g for boys and 46.3 ± 1.0 for girls) after adjustment for confounding variables (P < 0.0001 for both sexes). In the Westernized pattern, sugar intake was higher for most food sources, such as milk (7.2 ± 0.4 g for boys and 6.4 ± 0.3 g for girls), fruits (7.7 ± 0.7 g for boys and 9.1 ± 0.6 g for girls), and processed foods (36.7 ± 1.2 g for boys and 37.2 ± 0.8 g for girls), with commodity type foods being the exception. However, the contribution rate of sugar intake from each food source to total sugar intake was significantly different for processed foods and commodity type foods according to dietary pattern. Contribution rate of sugar intake from processed foods was higher for boys (P = 0.0199) and girls (P < 0.0001) in the Westernized pattern (65.3% for boys and 64.2% for girls), whereas contribution rate of sugar intake from commodity type foods was higher for boys (P < 0.0001) and girls (P < 0.0001) in the Traditional pattern (14.5% for boys and 12.7% for girls).
DISCUSSION
This study was conducted to estimate dietary sugar intake and relevant food sources according to sex using multiple-day dietary records for a large population of Korean children and adolescents. The average total sugar intake was 51.4 g/day (11.8%), and girls showed a higher total sugar intake than boys. The major source of sugars was processed foods, which accounted for > 50% of the total sugar intake. Frequent snacking and Westernized dietary pattern were associated with higher dietary sugar intake.
Total sugar intake of Korean children and adolescents was lower than that in Western populations. In Western countries, total sugar intakes were 139 g/day for subjects aged 1-18 years in the US [7], 97.4 g/day for subjects aged 4-10 years and 103.4 g/day for subjects aged 11-18 years in the UK [35], 124.6 g/day for subjects aged 9-13 years and 132.2 g/day for subjects aged 14-18 years in Australia [10], as well as 153.5 g/day for boys and 128.5 g/day for girls aged 9-13 years and 172.3 g/day for boys and 126.0 g/day for girls aged 14-18 years in Canada [36].
Our results are similar to those reported in other Korean studies. The average intakes of total sugars were 57.3-57.9 g per day for boys and 54.1-56.8 g for girls aged 6-19 years in 2001 [37] as well as 61.3-69.6 g for subjects aged 6-18 years between 2008 and 2011 [22] based on the Korea National Health and Nutrition Examination Survey, which used 1-day 24-h recall data.
We found that the major food source of sugars was processed foods. Among those, sweets and SSBs contributed to more than half of total sugar intake. As SSBs constitute the major food source for added sugars in Western countries, including the US, Brazil, and Canada [710111336], dietary sugar intake from processed foods should be monitored, particularly among adolescents, although total sugar intake in Korea was lower than that in Western countries.
The Westernized pattern was associated with higher total sugar intake than the Traditional pattern. The traditional Korean diet was composed mainly of white rice and kimchi, whereas the Westernized pattern was composed of various grains and grain products, fruits, milk and dairy products, and SSBs. The Westernized pattern in Asia may differ from the Western dietary pattern in US. The Westernized pattern in this study showed not only higher total sugar intake but also higher sugar intake from milk and fruits compared to the pattern in the US.
According to recent studies, associations of dietary sugars with obesity may differ depending on the food sources of dietary sugars. Two studies involving Korean children and adolescents reported an association between sugars from white milk or fresh fruits and reduced risk of obesity and BMI [3338]. Thus, milk and fruit intake and restricted SSB intake are recommended to maintain low sugar intake and prevent adverse health outcomes in Korean children and adolescents.
Most Korean children and adolescents in this study consumed at least one snack food during the study period. Due to rapid economic growth and globalization, the Asian diet has changed markedly over the past few decades to become Westernized, and the frequency of snacking and eating away from home has increased [2639]. Higher energy and sugar intakes from snacks in the Westernized pattern from our additional analysis can be understood in the same context. Accordingly, snacking should be regarded as an important factor in sugar consumption, especially in Korean children and adolescents.
The present study suggests that dietary sugar intake among Korean children and adolescents may be related to sex, dietary patterns, and snacking. A recent review reported relationships among diet, physical activity, and sedentary behavior [40], and Kim et al. [41] indicated that dietary behaviors, such as snack intake, were associated with lifestyle factors in Korean boys. In addition, snack and beverage consumption patterns differ according to sociodemographic status [42434445]. Therefore, a multilateral approach that embraces complex factors, including dietary behaviors, socioeconomic status, and lifestyle factors, is required to reduce dietary sugar intake and develop a nutrition education program for Korean children and adolescents.
This study has several limitations. First, this study used secondary data pooled from five studies. Although we collected all required information, including dietary records and sociodemographic variables, there may have been heterogeneity among the five studies. To lessen this bias, we used the study number as a confounding variable. Second, dietary sugar intake could be under-reported compared to other published data for Korean populations due to use of multiple-day dietary records. Finally, this study had a cross-sectional design, making it difficult to track changes in sugar intake in certain dietary patterns. Further prospective studies on the association between sugar intake and dietary patterns are thus warranted.
Despite these limitations, to our knowledge, this is the first study to examine dietary sugar intake and associations of dietary behaviors using multiple-day dietary records in order to estimate dietary sugar intake and relevant food sources in a large population.
In conclusion, the dietary sugar intake of Korean children and adolescents was higher in girls than in boys. The food sources of dietary sugars differed according to sex and dietary patterns. Multilateral and practical development of a nutrition education and intervention program that considers dietary behaviors as well as absolute sugar intake is required to prevent excessive sugar intake in Korean children and adolescents.






 XML Download
XML Download