

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder associated with several factors, such as genetic predisposition, lifestyle, and dietary characteristics [12]. The prevention of complications associated with diabetes, such as dyslipidemia, cardiovascular disease, renal dysfunction, and retinopathy [3], is of particular interest since these complications can confer a large burden on health care systems and increasing mortality rates [4]. The progression of diabetes is known to be caused by various modifiable lifestyle factors. Previous studies have reported that lifestyle modifications, such as restricting energy intake [5], maintaining a low carbohydrate diet [67], eating regular meals [8], increasing intake of high-fiber foods [9], maintaining a low sodium diet [10], avoiding excessive alcohol consumption, and maintaining a healthy weight [11], may delay or prevent complications of diabetes through near-normalization of blood glucose [12], blood pressure [13], and serum lipid levels [14]. In addition, early diagnosis of T2DM is critical in slowing the progression of this disease [15].
On the basis of epidemiologic observational studies and randomized trials, various recommendations for the management of T2DM have been developed [1617181920]. In 1990, the first South Korean recommendations for T2DM subjects were published by the Korean Diabetes Association (KDA) [16]. After 1990, these recommendations were updated in 1995, 2007, and 2011 in response to recent scientific evidence to emphasize the prevention and management of T2DM through lifestyle modifications [171819]. The most recent recommendations, updated in terms of food-based recommendations, were published by the Korean Ministry of Health and Welfare (KMHW) [20]. These recommendations have been distributed to both healthy subjects and those diagnosed with T2DM through books, brochures, and internet websites.
However, data evaluating the level of adherence to these recommendations among T2DM subjects are limited, particularly for South Korean subjects [21]. We therefore used the 1998 to 2012 versions of the Korea National Health and Nutrition Examination Survey (KNHANES) to evaluate trends in adherence to dietary and lifestyle recommendations among T2DM subjects. We also evaluated and compared adherence levels among patients with diagnosed and undiagnosed T2DM to determine if early diagnosis is associated with improvement in dietary habits and adherence to these recommendations. By doing so, we were able to test the hypothesis that the level of adherence to recommendations is higher among subjects diagnosed with T2DM than among undiagnosed subjects.
SUBJECTS AND METHODS
Population and design
This study analyzed data collected by the 1998-2012 KNHANES, a cross-sectional, nationally representative survey that collects extensive information through a health interview, health examination, and nutritional survey. Details of this survey can be found elsewhere [22]. Briefly, the survey used a complex, stratified, multistage, probability-cluster sampling of non-institutionalized Korean individuals of at least 1 year of age in South Korea. The KMHW established and conducted a series of three KNHANES in 1998, 2001, and 2005. Starting in 2007, KNHANES were carried out year-round to produce a timeline data, but no major changes to the questionnaires or methods of health examinations have been made since. All subjects in this survey provided written consent, and the study was approved by the Korea Centers for Disease Control and Prevention Institutional Review Board.
Of the potential 161,488 participants, individuals younger than 30 years (n = 64,232), those with missing information on sampling weight variables necessary for time-series analysis (n = 54,605), pregnant or lactating women (n = 362), and those who reported implausible total energy intake, i.e., < 25% or > 300% of the estimated energy requirements (n = 630) were excluded. Individuals with T2DM were included if they met at least one of the following conditions: (a) a fasting glucose level ≥ 126 mg/dl [23], (b) medical treatment with insulin or oral hypoglycemic medication, (c) a medical history of diabetes as diagnosed by a physician, or (d) self-reported T2DM. Those who gave positive responses to questions (b), (c), or (d) were defined as having diagnosed diabetes and the remainder were considered to have undiagnosed T2DM. A total of 4,955 participants were included in the final analysis (Fig. 1).
Measurements
A self-report questionnaire was used to collect demographic and lifestyle information, including age, sex, level of education, household income, smoking, alcohol intake, and experience with diabetes treatment or education for diabetes management. "Diabetes treatment" was defined as either pharmacological treatment with oral agents and/or insulin, or non-pharmacological treatment including diet modification and regular exercise. Anthropometric measurements were conducted by a trained technician. Body weight and height were measured in light clothing with no shoes, and body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Overweight/obesity was defined according to the 2000 statement from the World Health Organization for Asian populations, which defined the BMI cut-off value for overweight as 23 kg/m2 and that for obesity as 25 kg/m2 [24]. Self-administered physical activity questionnaires were administered as part of the KNHANES. However, as no physical activity questionnaires were conducted in 1998 and 2001, some details were omitted in 2005, and only 8% of participants responded in 2007, physical activity variables could not be used to examine recent trends. Alcohol intake level was calculated by multiplying the servings of alcohol consumed in one sitting by the frequency of consumption.
Dietary habits were examined, including how regularly basic meals (breakfast, lunch, and dinner on two consecutive days prior to the interview) were eaten on the basis of self-reported measures. Using this information, "regular meal pattern" was defined as subjects not skipping meals for two consecutive days. Vegetable and seaweed intake levels were assessed using a single 24-h dietary recall, and individual intake levels for each item were calculated, with the exception of kimchi and pickled vegetables, using the food code (variable names n_fcode, n_fname, nf_intk3). Serving sizes of food items were defined according to the Dietary Reference Intakes for Koreans [25].
Blood samples were taken in the morning after overnight fasting of at least 8 hours and sent to a certified laboratory for measurement of plasma glucose concentration. This analysis was performed by the Korea Association of Health Promotion (Hitachi 747 autoanalyzer; Hitachi, Tokyo, Japan) in 1998 and 2001. For this same analysis, a hexokinase method system (ADVIA 1650 system; Bayer HealthCare, Tarrytown, NY, USA) was used by the Central Testing Institute (Seoul, South Korea) in the 2005 and 2007 surveys, and from 2008 the hexokinase method (Hitachi 7600 autoanalyzer; Hitachi, Tokyo, Japan) was utilized by the Neodin Medical Institute (Seoul, South Korea).
Assessment of adherence level to dietary recommendations for T2DM
In this study, the components of dietary recommendations for T2DM were defined primarily based on the treatment recommendations for diabetes (2nd [17], 3rd [18], and 4th [19] editions) developed by the KDA, along with the dietary recommendations for disease management [20] published by the KMHW. Dietary guidelines according to the Dietary Reference Intakes for Koreans [25] were also incorporated in the development of the KDA and KMHW recommendations (the KDA-KMHW index). The level of adherence to the KDA-KMHW index was calculated based on the following 6 components: 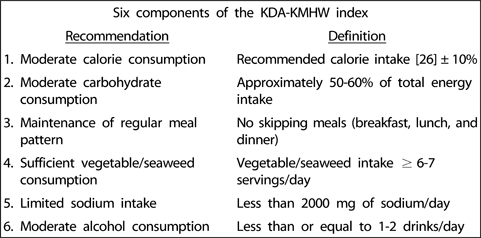
The participants received 1 point if they met the criteria for each of the 6 components, and the total possible score for the KDA-KMHW index ranged from 0 to 6 points, with a higher score indicating better adherence to recommendations.
Statistical analysis
Data were analyzed using the SAS statistical software package version 9.2 (SAS Institute Inc., Cary, NC, USA). All statistical analyses were conducted in accordance with survey procedures to account for the complex survey design, which consisted of multi-stage, stratified, clustered samples. For categorical variables, the chi-square statistic was computed to compare participant characteristics between survey years. The weighted means ± standard errors of continuous variables were estimated and compared between diagnosed and undiagnosed T2DM subjects and between survey years using the t-test, ANOVA, and generalized linear regression analysis. Multivariate regression analysis was performed with PROC SURVEYREG. Tests for trends were conducted by modeling the values as continuous variables. All tests were two-tailed, with the critical value for P set at α = 0.05.
RESULTS
Demographic and lifestyle characteristics of T2DM subjects
Between the 1998 and 2012 surveys, the prevalence of T2DM slightly increased from 11.8% to 13.1%, respectively, and the age of T2DM subjects significantly increased (Table 1, P < 0.001). The proportion of participants that were overweight or obese increased between 1998 and 2007 (from 65.5% to 76.4%), and then decreased between 2007 and 2012 (from 76.4% to 70.6%). Over the 14 years studied, smoking rates decreased by approximately 21.3% (P for trend < 0.001).
Increasing trend in the proportion of diagnosed diabetes cases
Fig. 2 shows the trend in the proportion of diagnosed cases in relation to the total number of T2DM subjects with either self-reported diabetes or fasting glucose levels ≥ 126 mg/dL over the survey years. Overall, the proportion of diagnosed diabetes increased dramatically from 40.9% in 1998 to 75.9% in 2012 (P for trend < 0.001), although these increments plateaued during the more recent survey years of 2007 to 2012.
Demographic and lifestyle characteristics of diagnosed and undiagnosed T2DM subjects
The average age and education level of diagnosed T2DM subjects were significantly higher than those of undiagnosed subjects for all survey versions (Table 2, P < 0.05), with the exception of education level for the 2007 and 2009 surveys. Diagnosed T2DM subjects tended to have a lower prevalence of current smoking than undiagnosed subjects, with statistically significant differences between the groups in 1998 (P = 0.02), 2008 (P = 0.002), and 2009 (P = 0.01).
Trends in adherence to each recommendation of the KDA-KMHW index among diagnosed and undiagnosed T2DM subjects
Fig. 3 shows the results of analysis of adherence to the 6 dietary recommendations for diagnosed and undiagnosed T2DM subjects from 1998 to 2012, adjusting for age, sex, BMI, education, household income, and smoking status. Overall, there were no significant differences in adherence to dietary recommendations between diagnosed and undiagnosed T2DM subjects for all survey years. No significant changes were observed over time regarding adherence to moderate calorie consumption, moderate carbohydrate consumption, or maintaining regular meal patterns for either the diagnosed or the undiagnosed subjects, whereas significant changes were observed regarding adherence to vegetable/seaweed, alcohol, and sodium intake guidelines. Adherence to sufficient vegetable/seaweed consumption increased over time for diagnosed subjects, specifically from 0.12 to 0.16 points (P for trend = 0.2), but not for undiagnosed subjects (P for trend = 0.2). Sodium intake for both diagnosed and undiagnosed subjects tended to improve over time, with adherence to limiting sodium intake increasing from 0.13 points in 1998 to 0.19 points in 2012 among diagnosed subjects (P for trend = 0.02) and from 0.12 points in 1998 to 0.24 points in 2012 among undiagnosed subjects (P for trend = 0.01). However, adherence to moderate alcohol consumption decreased over time for both diagnosed and undiagnosed subjects (P for trend < 0.05). The least-followed recommendations were moderating carbohydrate consumption (0.06-0.16 points), moderating total calorie intake (0.16-0.25 points), and limiting sodium intake (0.05-0.31 points), while the most-followed recommendation was maintaining regular meal patterns (0.62-0.84 points).
Trends in adherence to the KDA-KMHW index among diagnosed and undiagnosed T2DM subjects
Fig. 4 illustrates the trends in the KDA-KMHW index, which indicates the levels of overall adherence to recommendations, including the 6 dietary recommendation components, among both diagnosed and undiagnosed T2DM subjects. From 1998 to 2012, the KDA-KMHW index ranged 1.92-2.18 and 1.87-1.92 among diagnosed and undiagnosed subjects, respectively, and remained stable (P for trend = 0.8 for diagnosed subjects and = 0.9 for undiagnosed subjects). In addition, diagnosed T2DM subjects did not differ in adherence levels from undiagnosed subjects for all survey years (P > 0.05).
DISCUSSION
Our study found that overall adherence levels to dietary recommendations for T2DM, based on the KDA-KMHW index, were poor among Korean T2DM patients over the 14 years studied. However, while the level of adherence to T2DM-control recommendations did not significantly differ between diagnosed and undiagnosed T2DM subjects, the proportion of diagnosed subjects with sufficient vegetable/seaweed and limited sodium consumption increased, while the proportion of subjects with healthy drinking habits decreased between 1998 and 2012. This pattern was also observed for undiagnosed subjects, showing increased adherence to limiting sodium intake but decreased adherence to moderating alcohol consumption over time.
One of the least followed recommendations was moderating carbohydrate consumption, which is particularly important for T2DM subjects. Both diagnosed and undiagnosed T2DM subjects had a low level of adherence in limiting carbohydrate consumption to 50% to 60% of total energy intake, with only 10% to 20% of subjects following this guideline. This result was substantially lower in our study than in a study of European populations, which showed that more than 70% of T2DM patients adhered to limiting carbohydrate consumption to 50% to 60% of total energy intake [27]. A previous meta-analysis of 19 randomized clinical trials examining the association between a low-carbohydrate diet and various cardiovascular risk factors showed that limiting carbohydrate intake had favorable effects on body weight, BMI, abdominal circumference, systolic blood pressure, diastolic blood pressure, triglyceride level, fasting glucose level, insulin level, HDL cholesterol level, and C-reactive protein level [28]. In addition, a meta-analysis that analyzed data collected from T2DM subjects in 13 randomized clinical trials also suggested that maintenance of a low-carbohydrate diet results in beneficial health effects, including improvements in glycemic control and triglyceride levels [29]. As T2DM can be considered a disorder of carbohydrate metabolism resulting in hyperglycemia, lowering carbohydrate intake is critical for T2DM subjects [67]. However, carbohydrate intake is higher in the Korean population compared to other Asian and Western populations [30]. The average level of carbohydrate intake for Korean adults is approximately 73% of total energy intake [31], and Korean adults with T2DM have a high carbohydrate intake [32], as was observed in the current study. Korean adults, even diabetic patients, habitually consume a bowl of rice per meal as part of 2 or 3 meals per day [33], since rice is the predominant staple food and primary dietary source of carbohydrates in South Korea [34]. As there appears to be a wide gap between the current dietary guidelines and dietary practices, future efforts at development of dietary guidelines should account for cultural factors, and efforts to decrease carbohydrate intake to recommended levels and improve the quality of carbohydrates consumed (e.g., of whole grain content) by Korean diabetic patients should be continued.
Dietary guidelines recommend that patients with T2DM should limit sodium, but there are controversial aspects of these recommendations [17203536373839]. Higher dietary sodium intake is known to be associated with an increased risk of hypertension, a key risk factor for development of cardiovascular disease [3536]. However, some study results have shown that lower salt intake is associated with an increased risk of cardiovascular diseases and mortality [3738]. Ekinci et al. [38] examined the association between dietary salt intake and mortality in patients with T2DM, using 24-h urinary collections, and showed that lower levels of 24-h urinary sodium excretion were associated with an increase in all-cause and cardiovascular mortality. In addition, Maillot and Drewnowski [39] found that reducing sodium to below 2,000 mg/d is associated with sharp deviations from existing food patterns among independently living people. Thus, meeting this guideline may not feasible, and may pose challenges in meeting the requirements for multiple other nutrients. Currently, Korean nutrition policy promotes sodium reduction as the principal nutritional means of reducing blood pressure and its attendant cardiovascular disorders in adults. Our results showed that adherence to the recommendation to limit sodium intake to less than 2,000 mg/d was very low. Further research is clearly warranted to elucidate sodium's role in health and disease, and the results should be used to continuously update dietary guidelines using a practical, evidence-based approach.
The health effect of alcohol consumption among T2DM patients is also controversial. Basically, the Korea Ministry of Health & Welfare recommends that T2DM patients limit alcohol consumption since it is high in calories [20]. Prior studies have shown that moderate alcohol consumption (< 2 drinks/day) may lower the risk of T2DM complications by improving lipid, blood pressure, and fasting insulin levels [40], and the relationship between alcohol use and total mortality has been describe as a J-shaped or U-shaped curve [41]. However, recent reports indicate that alcohol consumption may cause hypoglycemia with glucose-lowering agents [42], and alcohol abstinence was linked with improvement in fasting glucose results among patients with glucose intolerance [43]. Our results showed that approximately half of diagnosed and undiagnosed subjects have adhered to the "moderate alcohol consumption" recommendation, consuming ≤ 1-2 drinks/day, but there were significant trends of decreasing adherence with time. This means that approximately half of diabetic patients consume more than 2 drinks per day, and that this proportion is increasing. Future studies are warranted to establish clear recommendations regarding alcohol consumption for essential management of T2DM, especially for Korean patients.
Overt T2DM is preceded by a long period of asymptomatic diabetes, during which hyperglycemia, hyperinsulinemia, and other features are present and complications have begun to develop [44]. Undiagnosed or unmanaged T2DM may hasten the development of diabetes complications, including macrovascular (ischemic heart disease, peripheral vascular disease, and cerebrovascular disease) and microvascular (retinopathy, nephropathy, and neuropathy) disorders [45]. In the current study, there was no clear evidence that diagnosed T2DM patients were significantly better at maintaining healthy dietary habits and lifestyle than undiagnosed subjects. This finding is in accordance with a previous finding that diabetes awareness was not associated with improved achievement of healthy cardiometabolic biomarker levels [46]. Nevertheless, the possibility that people with undiagnosed diabetes may be at greater risk for diabetic complications, including obesity, albuminuria, hypertension, and dyslipidemia [47], cannot be eliminated, as diagnosed T2DM subjects may have more opportunities to have regular medical check-ups and participate in health promotion programs [4849].
This study had several limitations. Although fasting blood glucose levels were measured to identify diagnosed and undiagnosed T2DM, the definition of diabetes was based on self-reported information that was not subjected to medical record validation, and thus diagnostic misclassification cannot be ruled out. Another limitation was that the analysis of trends was based on point prevalence rather than incidence, which is a better measure in terms of controlling for confounding factors such as survival time or disease duration. In addition, information on physical activity, a key part of managing T2DM, was unavailable, incomplete, or was asked differently from year to year between 1998 and 2007; thus, we could not adjust for physical activity levels in multivariate analyses. Finally, dietary information was obtained from a single 24-hour recall, which may not reflect habitual food intake. However, to our knowledge, this study was the first to describe trends in adherence to dietary recommendations among Korean T2DM subjects, while also considering the effects of disease awareness, by analyzing nationally representative data, thus allowing the findings to be generalized to all Korean diabetic patients.
In conclusion, Korean T2DM patients reported poor adherence to dietary recommendations and maintenance of a healthy lifestyle, regardless of disease awareness. The dietary guidelines should not be considered in isolation and should reflect understanding of their applicability to the food culture of a population using a practical, evidence-based approach. Following a diagnosis of T2DM, patients should be provided with more opportunities for participation in diabetes self-management education programs to learn how to manage glucose levels, maintain a healthy lifestyle, and prevent diabetes complications. Large-scale prospective cohort studies using validated measures of diabetes and collection of data over multiple days by unannounced 24-hour recalls or administration of well-validated food frequency questionnaires are warranted to confirm the findings.





 XML Download
XML Download