

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The common variants in fat mass and obesity associated gene (FTO) were first discovered in associations with type 2 diabetes [1] but were replicated by subsequent studies as susceptible loci associated with obesity [2-4] rather than with diabetes [5]. Successful replications of the association between variants in FTO and body weight have been demonstrated mainly among populations from European ancestry [2-5]. In particular, the rs9939609 single nucleotide polymorphism (SNP), which is located within the first intron of FTO, has been most extensively studied and was found to have a strong association with body mass index (BMI) [1,2,4]. However, findings on the associations of rs9939609 and further FTO SNPs with obesity have been inconsistent among Asian populations [5,6-12].
The prevalence of metabolic syndrome (MS) increasingly affects Asian adults and its prevalence ranges 10% to 19% [13]. Each of MS traits including obesity, dyslipidemia, high blood pressure, and elevated fasting glucose levels is well-known as a cardiovascular risk factor and the clustering of these features apparently elevates mortality of cardiovascular disease [14]. Although obesity and MS do not completely overlap, obesity is considered the core of MS and thus the FTO has been selected as a candidate gene related to MS in a study including European individuals [15]. On the basis of accumulated data on blood pressure and indicators of glucose and lipid metabolism, furthermore, carriers of the A-risk allele at rs9939609 are likely to have higher blood pressure [16,17], lower HDL cholesterol levels in blood [18-20], and higher blood glucose [20]. In contrast, some studies showed no association of the FTO variants with any MS trait as well as with the MS clustering [21-25]. There is only one prospective follow-up study by which a significant association between the FTO variants and the risk of MS was reported among Swedish individuals [15]. For Asian populations, however, there is currently a paucity of research for MS prevalence [18,25] and none for MS incidence in associations with the FTO variants. Furthermore, interactions between the FTO variants and lifestyle-related factors including smoking, alcohol drinking, sedentary lifestyle, and diet on MS incidence have not yet been evaluated so far. With genetic predisposition, sedentary lifestyle or higher intake of total energy and specific macronutrients may contribute to the development of MS.
The aim of present study was to investigate prospectively the future development of MS depending on the FTO rs9939609 genotypes and examine whether BMI and lifestyle-related factors modify the association between the FTO variants and MS incidence in population-based cohorts composed of Korean adults.
Subjects and Methods
Study population
The present study is based on two population-based prospective cohort studies, which are ongoing investigations embedded within the Korean Genome Epidemiology Study (KoGES) with a goal of conducting genome-wide association studies (GWAS). Detailed information on the population and method of each cohort study and the procedures of GWAS is available in previous reports [26,27]. One cohort study has been conducted at the Korea University Ansan Hospital and the other study at the Ajou University Medical Center. All members of both cohorts are Korean adults with the same ethnic background and were aged 40 to 69 years at baseline. The baseline examinations of both studies started from June 18, 2001 and were completed by January 29, 2003. During the site visit, all participated in a comprehensive health examination including anthropometric evaluation and collection of biospecimens for assays as well as in a questionnaire-based interview. They have been followed biennially up with a scheduled site visit for similar interviews and health examinations administered by trained health professionals. Major questionnaires including lifestyle-related factors and technical procedures of both cohort studies are periodically standardized. At each visit, participants sign an informed consent form, which was approved by the Human Subjects Review Committee either at the Korea University Ansan Hospital or at the Ajou University Medical Center.
For the study population of this investigation, we selected 5,459 individuals, who were free of metabolic syndrome or cardiovascular disease and who had acceptable genotype data that passed quality control and who provided information on lifestyle-related factors and adequate dietary intake (calorie intake that falls inside of five standard deviations), on the basis of baseline data.
Definition of the metabolic syndrome
The metabolic syndrome is defined as the presence of three or more of five traits including high concentrations of serum triglycerides (≥ 150 mg/dL or use of medications due to dyslipidemia), low concentrations of serum HDL cholesterol (< 40mg/dL for men and < 50 mg/dL for women), high blood pressure (systolic/diastolic pressure ≥ 130/85 mmHg or use of antihypertensive medications), and high concentrations of fasting glucose (≥ 100 mg/dL or use of medications due to elevated glucose) [28]. In addition, central obesity given as waist circumference is also considered a MS trait and defined as > 85 cm for men and > 80 cm for women. Such waist circumference cutoff points have been suggested to be optimal for MS diagnosis among Korean adults [29]. Because the data of follow-up examinations and interviews from April 17, 2003 to April 15, 2009 were technically validated, information on incident cases of MS as the outcome of present study was collected over 6 years.
Genetic and biochemical analyses
Genotyping of the FTO rs9939609 polymorphisms was carried out as part of GWAS procedure as reported in a previous study [12]. This published report provides detailed information on preparation of genomic samples, genotyping method, and quality control for data [12]. Briefly, participants had fasted for at least 8 hours before the beginning of blood collection for genotyping and biochemical analyses. Genomic DNA was collected from blood samples and 500 ng of DNA was processed according to the Affymetrix Genome-wide Human SNP array 5.0 (Affymetrix, Inc., Santa Clara, CA, USA). The genotyping call rates were greater than 95% and the genotype distribution of rs9939609 SNP was in Hardy-Weinberg equilibrium (HWE) (P-value = 0.31).
Biochemical assays for serum triglycerides and HDL cholesterol and plasma glucose were conducted at baseline as well as during the follow-up examinations. The laboratory reported inter-assay coefficient variations from routine assays; 5.2% for triglycerides, 3.8% for HDL cholesterol, and 2.8% for glucose.
Health examination and interview on lifestyle-related factors
Comprehensive health examinations and questionnaire-based interviews were periodically conducted. To evaluate obesity, participant's height (cm) and body weight (kg) were measured to the nearest 0.1 cm or 0.1 kg, respectively, and his or her BMI was calculated as weight in kilograms divided by height in meters squared. Waist circumference (cm) was measured at the narrowest part between the lower rib and the iliac crest to the nearest 0.1 cm and the average of three repeated measurements was calculated. Blood pressure was measured in a sitting position with mercury sphygmomanometers after at least a 5 minute period of rest. Repeated measurements of blood pressure were performed after about a 30 second interval and recorded to the nearest 2 mmHg. The average of measurements was calculated for systolic and diastolic blood pressure.
The questionnaire requested information on lifestyle-related factors such as smoking, alcohol drinking, physical activity, and dietary intake. The method of calculation for average daily alcohol consumption (g/day) and total metabolic equivalent scores (MET/hour) for physical activity has been described elsewhere [26]. Dietary information was collected using a semi-quantitative food frequency questionnaire (FFQ), which was developed by the Korea Centers for Disease Control and Prevention (Seoul, Korea). For the recall of food items or beverages consumed in the previous year, participants were asked to complete the FFQ table with inquiries about information on the average consumption frequency and serving size for 103 food items. During the interview with the FFQ, trained interviewers showed food pictures to help participants select serving size. On the basis of responses to the FFQ, average daily consumption of nutrients was calculated with food composition database published by the Rural Development Administration of Korea [30]. A previous study reported comparison of dietary intake by the FFQ and dietary record [31].
Statistical analysis
According to the FTO rs9939609 genotypes such as TT, TA, and AA, we calculated descriptive statistics for characteristics, which were examined at baseline. Distribution of categorical characteristics was evaluated by chi-square tests and continuous variables were compared by the analysis of covariance (ANCOVA) procedure with Scheffe's post-hoc tests. To test associations of the FTO genotypes and lifestyle-related factors with MS incidence, pooled logistic regression analysis was used. Compared with the major allele homozygote as a reference, the multivariate relative odds (RO), which is also called odds ratio, of MS incidence and its 95% confidence interval (CI) were obtained. If a 95% confidence interval does not contain 0, a P-value is considered less than 0.05. In multivariate models, covariates including age (continuous), sex, BMI (continuous), income (monthly wage of < 106 or ≥ 106 won), occupation (office job, non-office job, or others), educational level (< 9 or ≥ 9 years), smoking status (never smoker, former smoker, current smoker; < 10 cigarettes per year, 10-19 cigarettes per year, 20+ cigarettes per year), alcohol intake (abstainers, current alcohol consumption; < 15.1 g, 15.1-30, > 30 g/day), physical activity (quartiles of MET-hours/day), total energy intake (quartiles), energy-adjusted intake of carbohydrate or fat (quartiles), and study site were taken into account. To evaluate interactions between the genotypes and dichotomized variables of BMI (< 29 or ≥ 29 kg/m2) and lifestyle-related factors, such as smoking status (smoking or non-smoking), alcohol drinking (alcohol drinking or non-drinking), physical activity (the bottom quartile or other quartiles), total energy intake (the bottom quartile or other quartiles), and energy-adjusted intake of carbohydrate or fat (the bottom quartile or other quartiles), an interaction term for each of lifestyle factors was entered into logistic regression analysis. In interaction models, the TA and AA genotype groups were combined because the AA frequency was extremely rare. To investigate which MS component plays a more significant role in overall MS incidence, each of the components was included in MS cases as a requisite trait and then interaction models were fitted. All statistical analyses were undertaken using SAS program (SAS 9.1.3, SAS Institute, Cary, NC, USA).
Results
During a 6-year follow-up period, 1,487 cases (720 men and 767 women) of MS incidence were newly identified. Table 1 demonstrates characteristics of the study participants according to the FTO rs9939609 genotypes. Frequencies of the TT, TA, and AA genotypes were shown as 0.78, 0.21, and 0.02, respectively. The mean BMI was significantly higher in carriers with TA than in those with other genotypes. Demographic or lifestyle-related variables were not significantly different across the genotypes, although carriers with AA were younger and more likely to be physically active than those with TT and TA.
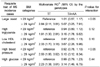
Tables 2 shows the association between the rs9939609 genotypes and MS incidence with results stratified by BMI. After taking into account age, BMI, and further potential risk factors of MS, no association was observed among all study participants, particularly among those with BMI less than 29 kg/m2. Among individuals with BMI of 29 kg/m2 or greater, however, carriers of the A-risk allele had a markedly significant increase in RO of MS incidence compared with non-carriers.
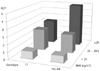
Fig. 1 demonstrates joint effects of the rs9939609 genotypes and BMI on MS incidence. Among individuals who had BMI less than 29 kg/m2, multivariate ROs of MS incidence were similar, regardless of the genotypes, within the same categories of BMI. In addition, carriers of the TT genotype with BMI of 29 kg/m2 or greater showed a RO similar to that observed among persons with BMI of 25 to 28.9 kg/m2; ROs (95% CI) were 2.91 (2.53, 3.34) for the TT carriers with BMI of 25 to 28.9 kg/m2, 3.30 (2.46, 4.44) for the TT carriers with BMI of 29 kg/m2 or greater, and 2.57 (2.08, 3.18) for carriers of the A-risk allele with BMI of 25 to 28.9 kg/m2 compared with the TT carriers with BMI less than 25 kg/m2. But, carriers of the A-risk allele with BMI of 29 kg/m2 or greater showed an approximately 6-fold higher RO (95% CI: 3.82 to 9.30) when using the same reference.
In Table 3, the associations of BMI and lifestyle-related factors with MS incidence are presented. As expected, increasing BMI was strongly associated with MS incidence. Heavy smoking as well as light to moderate smoking significantly elevated ROs of MS incidence. While light to moderate alcohol drinking did not elevate ROs, heavy drinking significantly did when compared with non-drinkers. Compared with individuals in the bottom quartile of physical activity, those in other higher quartiles showed about 15% reduced ROs of MS incidence. Total calorie intake and calorie-adjusted fat intake were not significantly associated with MS incidence. Compared with individuals in the bottom quartile of calorie-adjusted carbohydrate intake, those in other higher quartiles showed 22% to 29% reduced ROs of MS incidence after controlling for potential risk factors of MS.
Table 4 shows the effects of dichotomous variables of BMI and lifestyle-related factors on the association between the rs9939609 genotypes and MS incidence. BMI was dichotomized using 29 kg/m2 because this cutoff point was found to be a threshold beyond which significantly increased ROs of MS incidence. As presented in Table 4, BMI significantly modified the association between the rs9939609 variants and MS incidence (P-value for interaction < 0.05) while lifestyle-related factors did not. Regardless of the FTO genotypes, however, physical activity appeared to play a modifiable role in protecting MS occurrence because more active persons were likely to have lower ROs of MS incidence compared with those in the bottom quartile of MET-hours/day (Table 4).
Because only BMI was found to be a significant modifier, we further evaluated which MS trait is mainly influenced by the interaction between the rs9939609 genotypes and BMI. As indicated in Table 5, when MS clustering included either central obesity or high blood pressure as a requisite trait, BMI significantly modified the association between the genotypes and MS incidence (P-value for interaction < 0.05). Among obese persons with BMI of 29 kg/m2 or greater, carriers with the A-risk allele showed approximately 2-fold higher ROs of having high blood pressure trait compared with non-carriers even after taking BMI into account.
Discussion
A 6-year prospective cohort study including middle-aged and older Korean adults observed a significant association between the FTO rs9939609 variants and MS incidence only among obese persons with BMI of 29 kg/m2 or greater. After taking into account potential risk factors of MS, carriers of the A-risk allele at rs9939609 with BMI of 29 kg/m2 or greater showed an approximately 6-fold higher RO of MS incidence compared with the TT carriers with BMI less than 25 kg/m2. Compared with the same reference group, however, individuals with BMI of 29 kg/m2 or greater carrying the TT genotype showed a 3-fold higher RO, and those with BMI of 25 to 28.9 kg/m2 also showed similar magnitude in MS risk regardless of the genotypes. Thus, high BMI significantly modified the association between the rs9939609 variants and MS incidence, but lifestyle-related factors, including smoking, alcohol drinking, physical activity, and calorie intake did not.
The fat mass and obesity associated gene is located on chromosome 16q12.2 containing 9 exons and encodes a 2-oxoglutarate-dependent nucleic acid demethylase. Its postulated biological roles include the hypothalamic control of energy homeostasis [32] and food intake [33], the regulation of body fat content via adipocyte lipolysis [34], and cerebrocortical regulation of insulin [35]. Although this gene's genuine function in human obesity is still largely unclear, it is one of the most recognized genetic loci for the commonly occurring form of obesity. Several population genetic studies showed consistent replications [2-5], especially among populations from European ancestry, but studies for Asian populations reported conflicting data on the association with obesity [5-7] and obesity-related traits [23,25]. Ethnic discrepancies in previous findings may be partly due to low minor allele frequencies of the FTO variants. For example, the rs9939609 A-risk allele frequency ranges 12 to 20% in East Asians [6-8,10,12,18], while it is approximately 40% among populations from European ancestry [5]. In addition, lower levels of obesity in Asians than in other ethnic groups may have led to weak or null associations between the FTO variants and BMI [9]. Because of similar reasons, earlier studies among non-Caucasians, but not all studies, might have had limited statistical power to detect associations between the FTO variants and MS traits [23-25]. One study in the population with different non-Caucasian ethnicities demonstrated that carriers with the rs9939609 A-risk allele were more likely to have MS [18]. In our study, a null association between the rs9939609 SNP and MS incidence was observed among all participants, but a significantly elevated risk associated with carrying the A-risk allele was uncovered among persons with BMI of 29 kg/m2 or greater. Thus, only BMI was found as a significant modifier in the association between the FTO variants and MS risk. Our data suggest that not all carriers with the FTO risk allele become obese or diagnosed with MS. In particular, carriers of the A-risk allele with BMI of 25 to 28.9 kg/m2, which is in the range of obesity defined for Asians, did not show increased MS risks compared with non-carriers whose BMI was in the similar range. The effects of the A-risk allele appeared among persons with BMI 29 kg/m2 or greater. This fatness itself elevated the MS risk and further increased the risk when accompanied with a genetic factor such as having a FTO risk allele. On the basis of our findings, we speculate that there may be a threshold effect of BMI on the FTO variants in triggering certain metabolic disturbances and leading to MS incidence. Freathy et al. [20] reported that carrying the rs9939609 A-risk allele is significantly associated with higher triglycerides and lower HDL cholesterol, but not with LDL cholesterol. However, the significant association was nullified after adjustment of BMI [20] similarly shown in our findings. Instead, our results focusing on MS components imply that central obesity and high blood pressure may be potential components that underlie the association between FTO, BMI, and MS. Pausova et al. [17] hypothesized a biological role of FTO in the regulation of sympathetic vasomotor tone regarding the association between the FTO variants and blood pressure independent of BMI. Supporting this hypothesis, an experimental study showed that FTO-deficient mice keep leanness with systemic sympathetic activation [36] and an epidemiologic study observed a significant relation between the FTO variant and mortality due to diseases of the nervous system [37]. In addition, sympathetic vasomotor tone is elevated with hyperactivity of paraventricular nucleus neurons in the hypothalamus [38], where FTO is highly expressed.
Some, but not all [39,40], recent studies have demonstrated interactions between FTO and environmental factors, such as dietary intake [41] or physical activity [42,43], in association with obesity among adults. Sonestedt et al. [41] reported that energy-adjusted macronutrient such as fat or carbohydrate intake significantly modifies the association between the rs9939609 variants and obesity and suggested that FTO and high fat diet may exert synergistic effects on obesity. They have also pointed out that low physical activity may accentuate the genetic effects on the susceptibility of obesity as other studies similarly suggested [42,43]. So far, no data is available on the interaction between FTO and environmental factors in the association with MS incidence. One study has reported the association between the rs9939609 variants and MS incidence [15]. In the present study, we first convey data on the effects of a broad range of lifestyle-related factors on the association between FTO and MS incidence.
Several strengths and limitations need to be considered when our results are interpreted. Our study comprised population-based cohorts, which were derived from the well-defined homogenous population of Koreans, and used standardized methods to identify outcomes. Some limitations, however, are apparent. The follow-up rate for 6 years was 65%, but discrepancies in the distribution of BMI or the FTO polymorphisms were not significant between participants lost during follow-up and those kept in the long-term study. Our findings may not apply to other ethnicities, but may provide significant implications for Asians. Thus, further evaluations for other Asian groups are warranted. In addition, more data are called for to characterize the effects of other lifestyle-related factors, including detailed nutrient intake or obesity-related behaviors, on the association between FTO and MS risk. On the basis of our findings on the additive effects of smoking and sedentary lifestyle on MS risks regardless of the FTO polymorphisms, cessation of smoking and active lifestyle are recommended to reduce the MS risk as well as to prevent potentially cardiovascular disease. Moreover, because individuals who carry the FTO risk alleles and have BMI of 29 kg/m2 or greater, in particular, are considered a high risk population, they may need intensive weight loss regimens to prevent the development of MS.




 XML Download
XML Download