

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Kyung Seop Lee, Min Eui Kim1, Se Joong Kim2, Han Kwon Kim3, Hong Sup Kim4, Chun Il Kim5, Tae Gyun Kwon6 , Hyun Yul Rhew7, Kwangsung Park8, Dong Soo Park9, Jong Kwan Park10, Jae Shin Park11, Gyung Tak Sung12, Tae Hee Oh13, Sang Min Yoon14, Young Goo Lee15, In-Rae Cho16, Jin Seon Cho15, Jaeil Chung16, Hee Chang Jung17, Sung Hoo Hong18, Jae Seog Hyun19
, Hyun Yul Rhew7, Kwangsung Park8, Dong Soo Park9, Jong Kwan Park10, Jae Shin Park11, Gyung Tak Sung12, Tae Hee Oh13, Sang Min Yoon14, Young Goo Lee15, In-Rae Cho16, Jin Seon Cho15, Jaeil Chung16, Hee Chang Jung17, Sung Hoo Hong18, Jae Seog Hyun19
, Hyun Yul Rhew7, Kwangsung Park8, Dong Soo Park9, Jong Kwan Park10, Jae Shin Park11, Gyung Tak Sung12, Tae Hee Oh13, Sang Min Yoon14, Young Goo Lee15, In-Rae Cho16, Jin Seon Cho15, Jaeil Chung16, Hee Chang Jung17, Sung Hoo Hong18, Jae Seog Hyun19
Abstract
Purpose
The aim of this study was to identify the clinical baseline factors that affect failure of medical treatment (and especially surgical treatment) for benign prostatic hyperplasia (BPH) in spite of long-term medication.
Materials and Methods
802 men who were over 50 years of age with BPH were enrolled for this study. Patients were allocated to a medication group and a surgical treatment group (after having at least a 12 month duration of medication). We compared the differences between the two groups for their initial International Prostate Symptom Score (IPSS), the uroflowmetry, the prostate volume, the postvoid residual urine and the serum prostate specific antigen (PSA).
Results
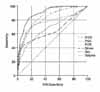
397 patients had surgical treatment following medication due to BPH progression (acute urinary retention, aggravating LUTS) and 405 patients were given maintenance medical treatment during follow-up. Statistically significant differences were found in the IPSS (23.3±6.6 vs. 12.7±8.4), the prostate volume (53.5±28.1ml vs. 38.3±12.6ml), the maximal flow rate (7.8±4.7ml/sec vs. 12.7±5.4ml/sec), the postvoid residual urine volume (92.7±144.4cc vs. 36.5±147.1cc), and the PSA (6.1±7.6ng/ml vs. 2.8±2.8ng/ml) between the surgical and medication groups. According to the area under the curve (AUC), the IPSS, prostate volume, maximal flow rate, postvoid residual urine volume and PSA are important in descending order. According to the receiver operating characteristic (ROC) curve-based prediction of the surgical intervention, the best cutoff value for the IPSS and prostate volume were 17 (area under ROC curve: 0.83) and 40ml (area under ROC curve: 0.68), respectively.
Figures and Tables
Fig. 1
Receiver operation characteristic of each parameters. IPSS: International Prostate Symptom Score, PSA: prostate-specific antigen, PVR: postvoid residual urine, Qmax: maximum urinary flow rate, QoL: quality of life.


References
1. Djavan B, Fong YK, Harik M, Milani S, Reissigl A, Chaudry A, et al. Longitudinal study of men with mild symptoms of bladder outlet obstruction treated with watchful waiting for four years. Urology. 2004. 64:1144–1148.
2. McConnell JD, Bruskewitz R, Walsh P, Andriole G, Lieber M, Holtgrewe HL, et al. Finasteride Long-Term Efficacy and Safety Study Group. The effect of finasteride on the risk of acute urinary retention and the need for surgical treatment among men with benign prostatic hyperplasia. N Engl J Med. 1998. 338:557–563.
3. Han KS, Hong SJ, Chung BH. Changing trends in the management of benign prostatic hyperplasia during recent 5 years. Korean J Urol. 2005. 46:458–462.
4. de la Rosette JJ, Kortmann BB, Rossi C, Sonke GS, Floratos DL, Kiemeney LA. Long-term risk of re-treatment of patients using α-blockers for lower urinary tract symptoms. J Urol. 2002. 167:1734–1739.
5. Djavan B, Chapple C, Milani S, Marberger M. State of the art on the efficacy and tolerability of alpha1-adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Urology. 2004. 64:1081–1088.
6. Kirby RS, Roehrborn C, Boyle P, Bartsch G, Jardin A, Cary MM, et al. Efficacy and tolerability of doxazosin and finasteride, alone or in combination, in treatment of symptomatic benign prostatic hyperplasia: the Prospective European Doxazosin and Combination Therapy (PREDICT) trial. Urology. 2003. 61:119–126.
7. Cha WH, Kim DG, Seo YJ, Lee KS. Comparison of treatment efficacy α blocker with finasteride and dutasteride in BPH. Korean J Urol. 2006. 47:Suppl. 179.
8. McConnell JD, Roehrborn CG, Bautista OM, Andriole GL Jr, Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003. 349:2387–2398.
9. Roehrborn CG, Bruskewitz R, Nickel JC, McConnell JD, Saltzman B, Gittelman MC, et al. Sustained decrease in incidence of acute urinary retention and surgery with finasteride for 6 years in men with benign prostatic hyperplasia. J Urol. 2004. 171:1194–1198.
10. Kim CI, Chang HS, Kim BK, Park CH. Long-term results of medical treatment in benign prostatic hyperplasia. Urology. 2006. 68:1015–1019.
11. Madersbacher S, Marszalek M, Lackner J, Berger P, Schatzl G. The long-term outcome of medical therapy for BPH. Eur Urol. 2007. 51:1522–1533.
12. Montorsi F, Moncada I. Safety and tolerability of treatment for BPH. Eur Urol. 2006. 5:Suppl. 1004–1012.
13. Djavan B, Waldert M, Ghawidel C, Marberger M. Benign prostatic hyperplasia progression and its impact on treatment. Curr Opin Urol. 2004. 14:45–50.
14. Hong SJ, Ko WJ, Kim SI, Chung BH. Identification of baseline clinical factors which predict medical treatment failure of benign prostatic hyperplasia: an observational cohort study. Eur Urol. 2003. 44:94–99.
15. Roehrborn CG. Alfuzosin 10 mg once daily prevents overall clinical progression of benign prostatic hyperplasia but not acute urinary retention: results of a 2-year placebo-controlled study. BJU Int. 2006. 97:734–741.
16. McNeill AS, Rizvi S, Byrne DJ. Prostate size influences the outcome after presenting with acute urinary retention. BJU Int. 2004. 94:559–562.
17. Roehrborn CG, McConnell JD, Lieber M, Kaplan S, Geller J, Malek GH, et al. PLESS Study Group. Serum prostate-specific antigen concentration is a powerful predictor of acute urinary retention and need for surgery in men with clinical benign prostatic hyperplasia. Urology. 1999. 53:473–480.
18. Kevin KM, Kattan MW. BPH serum markers and nomograms for selecting cnadidates for medical therapy. AUA news. 2005. 9:5–7.
19. Slawin KM, Kattan MW. The use of nomograms for selecting BPH candidates for dutasteride therapy. Rev Urol. 2004. 6:Suppl 9. S40–S45.
 XML Download
XML Download