

 PDF
PDF Citation
Citation Print
Print



Introduction
Cisatracurium, a stereoisomer of atracurium, is a non-depolarizing, benzylisoquinolinium intermediate-acting, neuromuscular blocking agent with 4 times the potency of atracurium. Cisatracurium decomposes into laudanosin and a tetravalent alcohol metabolite by Hofmann elimination in the blood plasma and extracellular fluid; hence, the recovery of muscle relaxation is hardly affected by diseases of the liver and kidney [1]. Due to these characteristics, cisatracurium has been used widely in managing intensive care unit patients, as well as in general anesthesia.
According to September 2013 data from Statistics Korea, the proportion of elderly people aged ≥ 65 years was 12.2%, a great increase compared with 3.1% in 1970; moreover, the rate is expected to further increase to 37.4% in 2050 [2]; accordingly, surgeries for the elderly that require general anesthesia are also expected to increase in number. Because of age-related changes in how the body processes medications, elderly patients are more sensitive to anesthetics, exhibiting side effects even with ordinary doses. In addition, the drug effects in this population are often prolonged [34]. Although a number of studies have compared the effects of muscle relaxants in the elderly, few have focused on the effective dose (ED) of cisatracurium and changes in the ED with aging in Koreans. We thus investigated the ED and onset time of cisatracurium for Korean adults aged 20 through 64 years and elderly Koreans aged ≥ 65 years.
Materials and Methods
The study was approved by the Clinical Ethics Committee, and informed consent was obtained from all patients before surgery. Among patients who were awaiting surgery after intubation under general anesthesia, adults were selected who were aged 20 through 64 years or aged ≥ 65 years and who had American Society of Anesthesiologists physical classifications 1 and 2, had no history of liver disease, renal disease, parathyroid disease, or hypercalcemia, and who had body mass indexes (BMI) of 18.5 to 24.9. Patients were excluded as test subjects if they were expected to bleed excessively, were scheduled for major surgery that would require massive hydration, were taking drugs (magnesium sulfate, lithium, antiepileptic drug) that would interact with non-depolarizing neuromuscular blocking agents, or would show adverse effects with the drug used in this study.
All patients received the following premedication after fasting since midnight: diazepam 5.0 mg orally, glycopyrrolate 0.2 mg and butorphanol 1.0 mg injected intramuscularly, and ranitidine 50 mg injected intravenously. Monitoring used the standard noninvasive method: attaching standard electrocardiograph electrodes II, a blood pressure measurement device, pulse oxygen saturation instrumentation and an end-tidal carbon dioxide concentration measurement device for all patients as they entered the operating room.
After anesthesia was induced with an intravenous injection of 2 mg/kg propofol (Propofol®, Dongkook Pharmaceutical Co., Seoul, Korea), it was maintained with an IV infusion of 5 mg/kg/h, and the depth of the anesthesia was confirmed by bispectral index. Oxygen was supplied through facial masks using 100% oxygen in a manual respirator, and end-tidal carbon dioxide concentration was maintained at 30–37 mmHg.
To assess muscle relaxation, the magnitude of relaxation (% control) was recorded using an acceleromyograph (TOFGuard®, Organon Teknika BV, Boxtel, Netherlands) as a peripheral nerve stimulator. The electrode was attached at a 7–11 mm range and 3–6 cm interval on the ulnar nerve travel site in the forearm on the opposite side from the blood pressure measurement device; each patient's deep body temperature was maintained at more than 35℃, and peripheral skin temperature was maintained at more than 32℃. Before muscle relaxants were administered, 50 Hz supramaximal tetanic stimulation was conducted for 5 seconds, and the response was stabilized with a 0.1 Hz single-twitch stimulus for 5 minutes; subsequently, thumb adductor spasmodic response was recorded with a 0.1 Hz the single-switch stimulus; after the stabilization, we selected 100% for the size of the single twitch. The effect of cisatracurium on a single twitch was calculated as percent reduction (= 100 - spasm size in percent).
A dose-response study on cisatracurium (Nimbex®, GlaxoSmithKline plc., Brentford, Middlesex, England) was conducted by measuring and recording the maximum muscle relaxation effect (% control) of the single twitch, as well as the time taken for the effect to reach the maximum after a randomly selected dose (from 30, 40, 50, 60 and 70 µg/kg) was administered within 5 seconds using a single bolus in 20 patients per dose in both adult and elderly patient groups. The relaxation effect and onset time were continuously monitored; the maximum relaxation effect was defined as the maximum calculated result, and the onset time was determined as the time to attain the maximum calculated result after confirmation that the relaxation had reached its maximum and had begun to decrease. After the study was complete, additional doses of cisatracurium were administered up to a total dose of 150 µg/kg, and intubation was performed after confirmation that the muscle relaxation had reached the maximum.
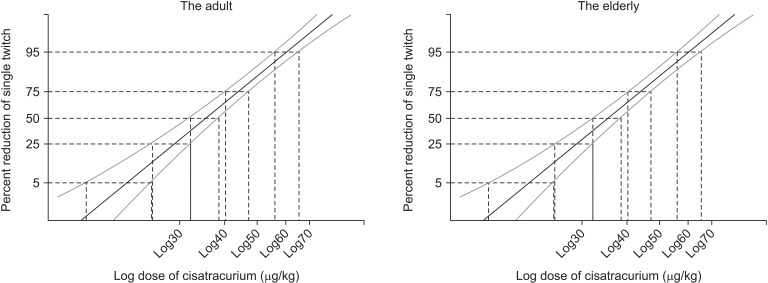
After each drug dose had been converted into a logarithm and percent reduction of the muscle relaxation into a probit, we estimated the effective doses for muscle relaxation effects of 5%, 25%, 50%, 75% and 95% using linear regression analysis. In the current study, we compared the ED values obtained by linear regression in which the reliability increased with the number of subjects, and the results for all 200 subjects, the 100 adult subjects and the 100 elderly subjects were all statistically significant. Age, height, weight, BMI and onset time were compared between the patient groups using ANOVA, with P value of < 0.05 considered statistically significant. All measurements are expressed as mean ± SD or 95% confidence interval.
Results
No statistically significant differences were observed in height, weight or BMI either within or between groups (Table 1A). Additionally, no statistically significant difference was observed in the maximum muscle relaxation effect by dose between the two groups (Table 2).
The estimated ED50 and ED95 for the total patient group were 35.11 (95% CI 32.65, 37.16) and 57.31 µg/kg (95% CI 54.40, 60.19), respectively. The ED50 and ED95 for the adult group were 35.39 (95% CI 31.76, 38.29) and 59.58 µg/kg (95% CI 55.46, 65.14), respectively, and the ED50 and ED95 for the elderly group were 34.89 (95% CI 31.28, 37.79) and 55.50 µg/kg (95% CI 51.90, 59.50), respectively (Table 3). There was no significant difference in ED50 or ED95 between the two groups.
The average onset time for the maximum muscle relaxation to appear was 375.4 ± 76.9 seconds in the adult group and 369.1 ± 70.0 seconds in the elderly group; no statistical difference was observed by age or administer dose (Table 4). Additionally, the slope of the dose-response regression line for cisatracurium did not deviate from parallel in either the adult or the elderly groups (Fig. 1).
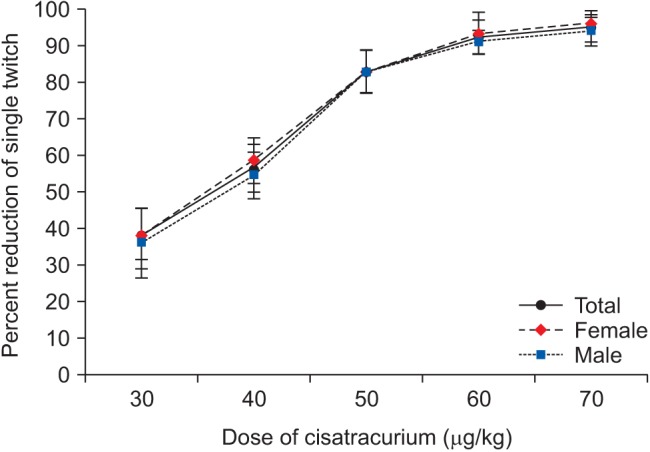
In addition, we compared the subjects by gender (Table 1B), and the mean maximum muscle relaxation by dose showed no significant gender difference (Fig. 2). However, a significant difference was observed in the ED95 by gender; the ED50 and ED95 for men were 35.79 (95% CI 33.34, 37.89) and 64.50 µg/kg (95% CI 61.07, 68.41), respectively, whereas the same two values for women were 34.47 (95% CI 30.74, 37.46) and 51.13 µg/kg (95% CI 47.63, 54.85), respectively.
Discussion
The proper use of neuromuscular blocking agents during surgery is necessary for surgical conditions. However, because incomplete recovery of muscle relaxation risks hypoxia, pulmonary complications, aspiration or airway obstruction, appropriate doses of these agents are very important. In a study by Maybauer et al. [5], the rates of residual paralysis following administration of cisatracurium and rocuronium were 57% and 44%, respectively.
Cisatracurium, a non-depolarizing, benzylisoquinolinium intermediate-acting, neuromuscular agent, decomposes into laudanosin and a tetravalent alcohol metabolite by Hofmann elimination. Because this decomposition occurs in the blood plasma and extracellular fluid, the recovery of muscle relaxation is little affected by liver or kidney diseases. Twenty-three percent of the dose depends on the organ, 16% of which is metabolized through the kidney. Studies on experimental animals found that cisatracurium was safer for the autonomic nervous system than were atracurium and vecuronium and that cisatracurium showed less secretion of histamine. No cardiovascular changes were observed with histamine secretion at 8 times the ED95 dose, and there was no increase in plasma histamine concentration when the doese was rapidly injected within 5 seconds. In addition, and similar to vecuronium, there was no change in the cardiovascular system with a double dose of ED95 administered to patients with coronary artery disease [16].
Aging is a biological process that causes progressive changes in the structure and function of organs. The size and blood flow of the kidneys decrease with aging, which affects drug metabolism and fluid and electrolyte regulation; in addition, liver volume and blood flow decrease with aging as well. Although age does not generally affect the pharmacodynamics of muscle relaxants, if medication depends on hepatic or renal metabolism, the duration of action can be extended. However, the metabolism of cisatracurium by Hofmann elimination does not depend on organ function, and thus, any effect on the duration of action is not significantly increased in the elderly [78]. Sagir et al. [9] compared the effects of cisatracurium with those of rocuronium and vecuronium among elderly patients and reported that cisatracurium was suitable for the elderly because it acted quickly. Arain et al. [10] also showed that cisatracurium was appropriate for elderly patients because of its more rapid activation and low variability in the recovery index.
We estimated the effective dose of cisatracuirum by linear regression analysis; the ED95 for the adult group was 59.58 µg/kg, and that for the elderly group was 55.50 µg/kg (Table 3). The P value was 0.562 following the homogeneity test between the estimated regression lines for the two groups, which indicated that the two lines were statistically homogeneous; furthermore, there was no significant difference in ED50 and ED95 between the adult and elderly groups (Fig. 1).
In the current study, the estimated ED50 and ED95 for the total patient group were 35.11 µg/kg (95% CI 32.65, 37.16) and 57.31 µg/kg (95% CI 54.40, 60.19), respectively. The results of our study differed from the 48 µg/kg that was estimated as the ED95 of cisatracurium by Belmont et al. [11] and the ED50 and ED95 of, respectively, 30 and 53 µg/kg found by Lepage et al. [12]. Geographic location and race are known to influence the potency and duration of drug action. Dahaba et al. [13] found a significant difference in rocuronium potency and duration of action among patients in three countries; however, they also showed that there was no difference between Chinese and Caucasians in the comparative dose-response and time-course of cisatracurium activity [14]. The differences between the EDs in our study and those from existing studies [1112] could be based on whether nitrous oxide was used. Nitrous oxide exhibits drug-drug interactions that strengthen the effects of neuromuscular blocking agents [1516]; in particular, the two existing studies used nitrous oxide to maintain anesthesia compared with the propofol alone that we used to maintain anesthesia in this study.
Arain et al. [10] studied onset time, duration of action and recovery index time for rocuronium and cisatracurium among both adult and elderly patients, and they found that cisatracurium showed no significant difference between the two groups. In a study by Sorooshian et al. [17] the authors observed that a bolus dose of cisatracurium caused marginally greater neuromuscular block in young patients compared with elderly patients and that the block developed more slowly in the elderly; however, the duration of neuromuscular block was similar in both groups of patients. The authors of the study also compared the pharmacokinetics and pharmacodynamics of cisatracurium between adults and the elderly and reported a slight difference between the two groups. Kisor and Schmith [18] reported minor differences in the pharmacokinetics of cisatracurium besilate in various patient populations because of the unique relationship between plasma clearance and volume of distribution because the primary elimination pathway for cisatracurium besilate does not depend on organ function. In addition, a study by Ornstein et al. [19] showed only minor differences in the pharmacokinetics of cisatracurium between elderly and young patients; similarly, the ED and the onset time in our study were not significantly different between the adult and elderly groups.
However, Joomye et al. [20] studied cisatracurium consumption and recovery index by age group—20–45, 46–64 and ≥ 65 years—and there were significant differences between the groups aged 20–45 and ≥ 65 years, likely because of the reduced body fluid that accompanies aging and that results in increased serum blood drug concentrations and increased volume of distribution due to increased body fat; the authors of that study suggested that the elderly require less cisatracurium to achieve a desirable effect. Although those authors reached their conclusion using consumption and recovery indexes with a closed-loop computer-controlled infusion, we investigated the cisatracurium ED and onset time with a single bolus. Furthermore, we classified the patients in this study into two groups, < 65 years and ≥ 65 years. In a review by Cope and Hunter [7], the effects of physiological changes on the pharmacokinetics of neuromuscular-blocking agents did not become clinically apparent in healthy individuals of at least age 75. In our current study, the average age in the elderly group was 71.4; we consider it a limitation of our study that it was not possible to clearly distinguish age differences between the groups. The ED50 and ED95 for the adult group were, respectively, 35.39 and 59.58 µg/kg, whereas the ED50 and ED95 for the elderly group were 34.89 and 55.50 µg/kg, respectively; although there were no statistical differences, there were still numeric gaps between the two groups. Thus, the topic warrants additional studies that are strictly designed with significantly more participants and distinct age differences between groups.
In addition, we estimated effective doses for men and women. For men, ED50 and ED95 were 35.79 (95% CI 33.34, 37.89) and 64.50 µg/kg (95% CI 61.07, 68.41), respectively, and those for women were 34.47 (95% CI 30.74, 37.46) and 51.13 µg/kg (95% CI 47.63, 54.85), respectively. The homogeneity test of the estimated regression line showed a P value < 0.05, which means that the two regression lines were not homogenous and the ED95 confidence intervals did not match. In a study by Xue et al. [21], women were 30% more sensitive to rocuronium than were men. Additionally, Shi and Liang [22] found a significant difference in the effective dose of cisatracurium between men and women, with ED95 of 67.4 ± 4.4 and 48.7 ± 1.0 µg/kg, respectively. Although men showed higher proportions of body fluid and blood plasma, the distribution volume was expectedly lower in women; furthermore, men generally have more muscle mass and less fat, and hence women are expected to be more sensitive to muscle relaxants. A study by Adamus et al. [23] showed that the onset time and clinical duration of rocuronium were shorter in women than men, whereas those of cisatracurium did not differ between the two groups.
The times taken to reach maximum muscle relaxation were 375.4 ± 76.9 seconds and 369.1 ± 70.0 seconds in the adult group and elderly groups, respectively, with no statistically significant difference, and the results by dose also showed no statistically significant difference (Table 4). Lepage et al. [12] reported cisatracurium onset times of 6.7 (1.8, 9.3), 5.8 (3.3, 6.3), 6.7 (2.8, 12.5) and 7.7 (5.5, 8.5) minutes for 25, 30, 40 and 60 µg/kg, respectively, without statistical significance.
In summary, in this study, the ED50 and ED95 for cisatracurium in Korean adults and elderly persons were 35.11 (95% CI 32.65, 37.16) and 57.31 µg/kg (95% CI 54.40, 60.19), respectively. The ED and the onset time were not statistically different between the two groups, but a significant difference was observed between men and women in ED95 only.
 XML Download
XML Download