

 PDF
PDF Citation
Citation Print
Print


Introduction
The safety margin of endotracheal tube (ETT) cuff pressure is determined between over-inflation and under-inflation. Under-inflation can cause air leakage, which lessens the effect of mechanical ventilation and produces a leakage of inhalation anesthetics. ETT cuff pressure below 20 cmH2O is a risk factor of ventilator associated pneumonia [1,2]. However, over-inflation of the ETT cuff can cause a serious injury and affect blood flow to the tracheal mucosa [3], resulting in tracheal stenosis, tracheoesophageal fistula, or tracheal rupture [4].
The tracheal intubated ETT can be displaced by movement of the patient's head and neck [5]. Movement of the head and neck and the displacement of ETT can cause a change in ETT cuff pressure [6,7]. There was a report on the effect of position change from spine to prone on cuff pressure [8], but the prone position in the study was with the patient's head rotated to the right. The purpose of this study was to evaluate the ETT cuff pressure by a position change to prone without the movement of head and neck. Additionally, the change in cuff pressure on flexion and extension of the patient's head was also evaluated.
Materials and Methods
This prospective and interventional study was approved by the Institutional Review Board of our hospital. Informed consent was obtained from all patients who were enrolled in the study. Fifty-five patients, 20 years or older and American Society of Anesthesiologists physical status 1-3, were enrolled and scheduled for lumbar spine surgery under general anesthesia. Exclusion criteria included patients with neck pain, a history of neck surgery, a limitation of neck movement, or morbid obesity (body mass index > 35).
The induction of anesthesia was performed with propofol, rocuronium, remifentanil (with target controlled infusion), and sevoflurane. All patients were intubated with a reinforced ETT (Mallinckrodt™, Covidien, Tullamore, Ireland), of inner diameter 7.5 mm for male, and 7.0 mm for female, when train-of-four (TOF) count was 0. TOF count was maintained at 0 during the study. The tip of the ETT was placed at 4 cm above the carina using a fiberoptic bronchoscope (FI-7RBS, Pentax Corp, Tokyo, Japan), and the cuff was inflated by the standard technique. The ETT was taped at the right corner of the patient's mouth with oral airway for bite block. Patients were mechanically ventilated by volume-controlled ventilation with 50% of oxygen in medical air. Initial tidal volume and respiratory rate was set at 8 ml/kg and of 10 cycle/min, respectively and adjusted to maintain less than 25 cmH2O peak airway pressure and an end-tidal carbon dioxide tension from 30 to 35 mmHg.
The patient's head and neck were postured straight and natural with a 5 cm high pillow, and this head posture was defined as a neutral posture. In neutral posture, the neutral angle, an angle on the mandibular angle between the midline of neck and the inferior border of mandible, was measured with a protractor (Fig. 1). The initial neutral pressure of the ETT cuff, inflated by the standard technique, was measured using a manometer (Mallinckrodt Medical, Hennef, Germany); subsequently, the cuff pressure was adjusted at 26 cmH2O. An ETT cuff pressure of 20 to 30 cmH2O was recommended to prevent the complication of under- or over-inflation, in previous studies [2,9]. The median values adjustment from 20 to 30 cmH2O was ideally 25 cmH2O, however, we set the cuff pressure as 26 cmH2O because our analog manometer was adjustable by 2 cmH2O intervals. When the posture of the patient's head was gently flexed, the flexed pressure of the cuff and the flexed angle were measured. The head posture was then returned to the neutral posture and the cuff pressure was re-adjusted to 26 cmH2O. The extended pressure of the ETT cuff and the extended angle were measured at the extended posture of the patient's head, and the patient's head was then returned to neutral posture. The cuff pressure was re-adjusted to 26 cmH2O in neutral position, before changing the position to prone. The position change from supine to prone was made on a Wilson frame with a standard operation table. The increase in intrathoracic pressure by the increased abdominal pressure in prone position was prevented by attempts to ensure that the abdomen of the patient was not compressed. The initial neutral pressure of cuff and the neutral angle were recorded in prone position, while the patient was kept at neutral posture in supine as possible. The flexed and extended pressure and angle were measured and recorded. The cuff pressure was measured after a steady period of 2-3 respiration cycles, with the values was recorded at end-expiration to minimize the effect of airway pressure. During the procedure, the manometer was continuously attached to the pilot balloon of the ETT, and the pressure was controlled by the pressure relief valve and bulb (manual pump) of the manometer. The pressure was decompressed right after the measurement for the patient's safety, if the cuff pressure was increased to more than 30 cmH2O.
The sample size was calculated based on the results of a previous study [8], and the standard deviation of cuff pressure in prone position with head rotation was 7.3 cmH2O. However, since our study aimed to evaluate the ETT cuff pressure by the position change to prone without the movement of head and neck, we presumed the standard deviation of ETT cuff pressure was 10 cmH2O, and a change of 5 cmH2O of cuff pressure was considered as significant. Accordingly a sample size of 44 patients was required to achieve a power of 0.9 and an α of 0.05. When the elimination rate was set at 20%, the valid sample size was calculated as 55 patients.
Data were expressed as mean ± SD or number of patients. Neutral, flexed, and extended angle were compared between supine and prone position. Initial neutral pressure in prone was compared with the adjusted neutral pressure (26 cmH2O) in supine. Flexed and extended pressure were compared with adjusted neutral pressure in supine or prone, respectively. The changes of angle and pressure were analyzed by paired t-test with two-tailed. The analysis was performed with SigmatPlot 12 (Systat Software Inc., San Jose, USA). Statistical significance was considered at P < 0.05.
Results
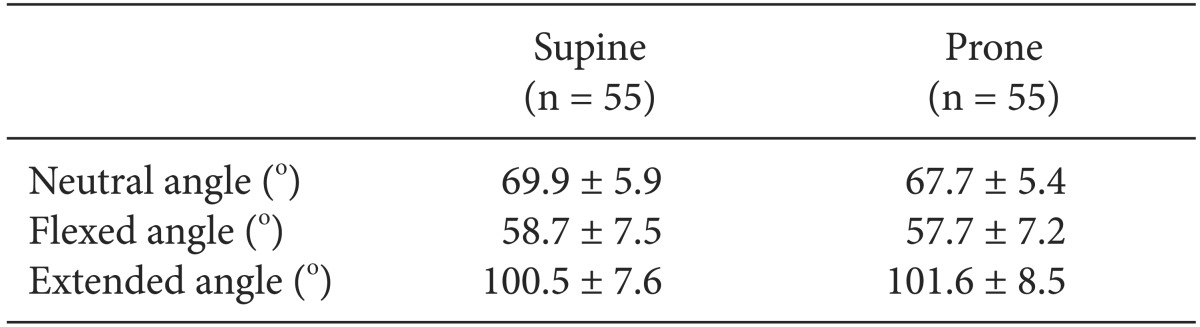
The age, sex, height, and weight of all patients were 58.6 ± 13.7 yr, 32 male and 23 female, 162.8 ± 8.9 cm, and 64.9 ± 9.9 kg. The neutral, flexed, and extended angle on the mandibular angle between the midline of neck and the inferior border of mandible were showed in Table 1. There were no differences between supine and prone position in neutral, flexed, and extended angle, respectively.
The initial neutral pressure was 32.4 ± 12.9 cmH2O at neutral posture when an ETT cuff was inflated by the standard technique in supine position. The initial neutral pressure after changing position from supine to prone was increased to 31.5 ± 5.9 cmH2O (P < 0.001) than the adjusted neutral pressure of the supine position (Table 2).
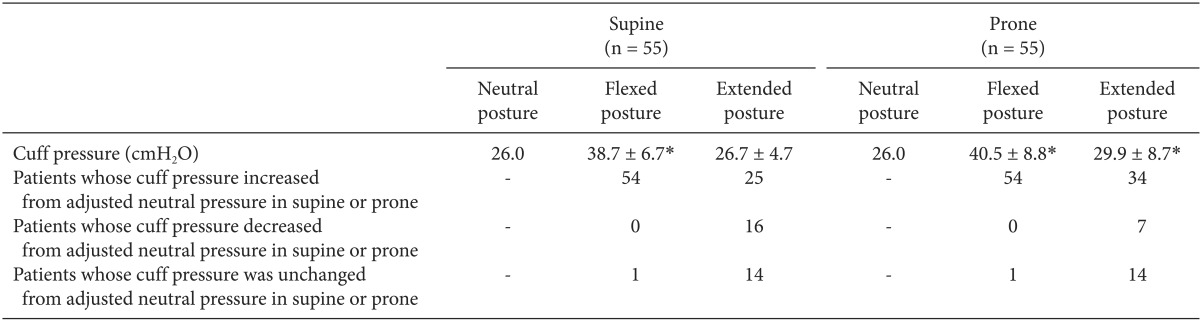
The flexed pressure in supine was significantly increased to 38.7 ± 6.7 cmH2O (P < 0.001) than the adjusted neutral pressure; and the extended pressure was not statistically changed than the adjusted neutral pressure (Table 3). After changing position from supine to prone, flexed and extended pressure were increased to 40.5 ± 8.8 (P < 0.001) and 29.9 ± 8.7 (P = 0.002) cmH2O than the adjusted neutral pressure, respectively (Table 3). The number of patients, whose cuff pressure was increased, decreased, or not changed, were presented in Tables 2 and 3. The maximum flexed pressure was 64 cmH2O in supine and 72 cmH2O in prone position, and the maximum extended pressure was 38 and 60 cmH2O in supine and prone, respectively.
Discussion
The results of this study demonstrated that position change from supine to prone increases the cuff pressure of ETT. Head flexion is a cause of increased cuff pressure in both supine and prone positions, but head extension increases the cuff pressure in the prone position only.
The position change to prone increased the ETT cuff pressure in our study (Table 2). We kept the posture of the head and neck unchanged in supine and prone positions, so that there was no difference between the neutral, flexed, and extended angles in supine position and those in prone position. The flexion of head and neck moves the ETT toward the carina, while extension displaces the tube cranially [5,10]. Kako et al. [6], showed that the cuff pressure was changed by head rotation, neck flexion and extension in a pediatric population, and the major cause of increased cuff pressure was movement of the ETT. Minonishi et al. [8] reported that supine-to-prone position change with head flexion and rotation resulted in decreased ETT cuff pressure and tendency of ETT withdrawal. They observed a significant correlation between ETT movement and change in cuff pressure. However, the head of patient was rotated to the right in prone position, which differed from our study. The main result of our study was that the cuff pressure increased from 26 cmH2O to 31.5 ± 5.9 cmH2O by the position change from supine to prone without any change in head and neck posture.
The cause of cuff pressure increase cannot be explained precisely, because the factors that affect the ETT cuff pressure in prone position have not been studied up to now. However, 2 factors can be postulated for the increased ETT cuff pressure by the position change only from supine to prone. The first is an anatomic structure of the neck. The trachea is located in the anterior portion of the neck, and therefore cervical spine, muscles, and major vessels can compress the trachea by the gravity in prone position [11]. Moreover, the trachea contains numerous rings of hyaline cartilage which are C-shaped and incomplete dorsally, so the posterior aspect of the trachea can be more easily compressed. The second factor for increased ETT cuff pressure is the increased intrathoracic pressure by the prone position with Wilson frame, because the anterior wall of the chest and abdomen is compressed. The increased intrathoracic pressure leads to an increasing airway pressure, which could cause the increase of ETT cuff pressure during inspiration, in patients with mechanical ventilation. However, during expiration, if a patient did not receive a positive end-expiratory pressure, the airway pressure decreased to near zero. In this study, because the cuff pressure was measured at the end-expiratory phase to prevent the effect of increased airway pressure in prone position, the effect of airway pressure would minimally increase the cuff pressure. The factors mentioned above are hypotheses that require further studies.
The cuff pressure was changed by the movement of head in our study, similar to the results of previous studies [6,7]. Flexed pressure increased from 26 cmH2O to 38.7 ± 6.7 cmH2O in supine and from 26 cmH2O to 40.5 ± 8.8 cmH2O in prone, while the flexed angle decreased about 10° than the neutral angle. When extended angle was increased about 30° than neutral angle, extended pressure was unchanged in supine but 29.9 ± 8.7 (P = 0.002) cmH2O in prone compared with neutral pressure. Although the flexed pressure and extended pressure were not directly comparable because the cuff pressure was re-adjusted in neutral posture before the change of head posture in this study, the flexed pressure was increased in 54 of 55 patients in both supine and prone positions. On the other hand, the extended pressure was increased in 25 patients in supine and 34 patients in prone. Therefore, flexed posture should be of more concern in clinical anesthetic management. Also, in the case of the combination of prone position and head flexion, an increased cuff pressure is expected. Overpressure of the ETT cuff can cause ischemic injury to the tracheal mucosa, hence the cuff pressure should be monitored and managed properly. The maximum flexed pressure was 64 cmH2O in supine and 72 cmH2O in prone position in our study, and tracheal rupture is possible even at these pressures [4].
The under-inflation of the ETT cuff can lead to air leakage, which lessens the effect of mechanical ventilation and produces the leakage of inhalation anesthetics. Rello et al. [1] reported that persistent intracuff pressure below 20 cmH2O has a high risk of ventilator associated pneumonia in intensive care patients. Extended pressure was decreased in our study than neutral pressure in 16 and 7 of 55 patients in supine and prone, respectively. Most of these patients had extended pressure above 20 cmH2O. However, if the neutral pressure was less than 26 cmH2O, the cuff pressure by the extension of head and neck could possibly be less than 20 cmH2O.
This study had some limitations. Firstly, we did not evaluate the displacement of the ETT after position change by fiberoptic bronchoscopy. The tip of ETT in supine position is not assuredly the same as that in prone position. Also, it is not clear whether the displacement of ETT occurs in flexed or extended postures. Secondly, in our study, neutral, flexed, and extended head posture in prone was not exactly the same as those in supine, which may have affected our results. However, we minimized differences of neutral, flexed, and extended head posture before and after changing the position to prone. Thirdly, because the mode of the manometer was not digital, there may have been an error in the reading of cuff pressure by the investigator. These factors might be a possible source of bias.
In conclusion, the position change solely from supine to prone without the movement of head and neck can cause the increase of endotracheal tube cuff pressure. Also, the head flexion leads to increased cuff pressure in most patients. Therefore, the cuff pressure of the endotracheal tube should be monitored and managed properly after the position change from supine to prone.


 XML Download
XML Download