

 PDF
PDF Citation
Citation Print
Print


Introduction
Propofol (2,6-diisopropylphenol), an intravenous hypnotic, has gained popularity as an agent for both induction and maintenance of anesthesia due to its rapid onset, short duration of action, and minimal side effects. The currently used long-chain triglyceride (LCT) emulsion propofol formulations have several drawbacks including inherent emulsion instability, need for antimicrobial agents, hyperlipidemia, pancreatitis, and pain on injection [1-4]. This has led to the development of improved formulations for this compound [5].
A lipid-free microemulsion propofol (Aquafol®; Daewon Pharmaceutical, Seoul, Korea) was developed to eliminate lipid solvent-related adverse events of LCT emulsion propofol. Microemulsion propofol demonstrated similar pharmacokinetics and pharmacodynamics to lipid emulsion propofol [6]. It has also been reported that microemuslion propofol is as effective and safe as lipid emulsion propofol [7]. However, microemulsion propofol produces more frequent and severe pain upon injection than lipid emulsion propofol and the significantly higher incidence and severity of pain on injection with microemulsion propofol is associated with a higher aqueous free propofol concentration [7,8]. In one study, 70% of patients who received microemulsion propofol reported considerable pain on injection [8].
There are a number of studies on the pharmacologic and nonpharmacologic strategies for the prevention of pain on propofol injection. They include premedication [9], cooling or diluting of the propofol solution [10,11] and concomitant therapies using ketamine [12], local anesthetics [13], ondansetron [14], and opioids [15,16]. However, despite various methods to reduce propofol injection pain, none of these have achieved the complete elimination of pain. Previous studies show that multimodal analgesia using different analgesic modalities can reduce the incidence and severity of propofol injection pain [17-19]. Also, a recent study shows that the combination of remifentanil and lidocaine was more effective in reducing the incidence of pain upon the injection of microemulsion propofol than either treatment alone [20].
The aim of the present study was to evaluate the effect of a combination of pretreatment with different doses of remifentanil and premixing of lidocaine on the incidence and severity of microemulsion propofol injection pain in adults undergoing elective surgery.
Materials and Methods
This study received Institutional Review Board approval, and informed consent was obtained from each patient. A total of 160 patients, aged 20 to 65 years, who were scheduled for elective surgery with general anesthesia and were American Society of Anesthesiologists (ASA) status I and II, were enrolled. Patients who had known allergy to any drugs; had renal, hepatic, or cardiac problems; had asthma, diabetes mellitus, neurologic deficits and psychiatric disorders; required a rapid sequence induction; or had received analgesics or sedatives within the 24 hours previous to enrolment were excluded.
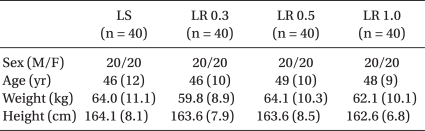
The patients were randomly assigned to one of the four groups according to the dose of remifentanil using an Excel (Microsoft, USA) generated randomization table. The four groups were comparable with respect to patient characteristics (Table 1). No patient was excluded from the analysis due to complications and therefore data for all 160 patients is presented.
The patients received saline (LS group, n = 45), remifentanil 0.3 µg/kg (LR 0.3 group, n = 45), remifentanil 0.5 µg/kg (LR 0.5 group n = 45), or remifentanil 1.0 µg/kg (LR 1.0, group n = 45) over a 30 s period, and 90 s later received an injection of 2 mg/kg microemulsion propofol premixed with lidocaine 40 mg over a 60 s period. Saline and remifentanil were prepared in a 10 ml unlabeled syringe by individuals who had not participated in the induction of anesthesia. Microemulsion propofol was mixed with 2 ml of 2% lidocaine. The patients, anesthesia providers and investigators who scored the movements were blinded to the treatment group. All study drugs were prepared before the injection at room temperature.
Before arriving at the operating room, a 20 gauge cannula was inserted in the left cephalic vein of the patient's nondominant hand, and its position was confirmed by the free flow of Hartmann's solution infused by gravity. Standard monitoring, including noninvasive arterial pressure, ECG, pulse oximetry and bispectral index score (BIS) monitoring was applied and assessed continuously. Before induction of anesthesia, all patients were preoxygenated. After remifentanil or saline injection, microemulsion propofol 2 mg/kg was administered through the rubber port connected to the intravenous cannula without the carrier fluid. The assessment of pain was made continuously from the start of the propofol injection to when patients lost their consciousness. The severity of pain was assessed using a four-point scale. Pain manifestation as a verbal response accompanied by facial grimacing or withdrawal of arm was scored as severe; grimacing or withdrawal not accompanied by a verbal response was scored as moderate pain. If severe or moderate pain was not observed, the patient was asked whether they had any discomfort in the arms; if they answered 'yes', this was scored as mild pain; if they answered 'no', this was scored as no pain [21]. After the loss of an eyelash reflex, the patients were intubated after administration of rocuronium 0.8 mg/kg. Anesthesia was then carried on normally.
After the remifentanil or saline injection, BIS score was checked to subjectively assess the level of consciousness to ensure an adequate response to the pain questionnaires. The mean arterial pressure and heart rate were recorded before injecting the study drug (baseline), after the remifentanil injection, and before tracheal intubation. Chest wall rigidity, described as transient chest discomfort, was also recorded during remifentanil injection. Patients were monitored hourly for 24 hours post-surgery by a blinded investigator for adverse effects at the injection site such as pain, edema, wheal and flare response.
Based on previously published data, the incidence of pain on injection of microemulsion propofol should be approximately 70% [8]. A reduction of 30% (from 70% to 40%) in the treatment group would be considered clinically important. Therefore, 37 subjects per group would be needed to decrease this incidence to 5% (power 80% and α = 0.05). We assumed a dropout rate of 10% and so increased the sample size to 40 patients per group.
Statistical analyses were performed using SPSS software (version 16.0, SPSS Inc., IL, USA). Analyses of variance were performed on the demographic data, using the one-way ANOVA test and the chi-square test. The chi-square test was used to calculate differences between groups in incidence of microemulsion propofol-induced pain. Differences in the pain scores among the groups were analysed with the Kruskal-Wallis rank test and Mann-Whitney tests were performed as post-hoc test among the groups. P value < 0.05 was considered significant. All values are expressed as mean (SD) or absolute numbers (%).
Results
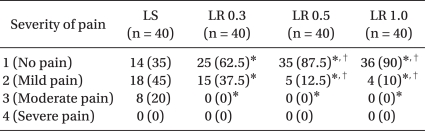
The overall incidence and intensity of pain during injection of microemulsion propofol in the groups is shown in Table 2. The incidence of pain from the microemulsion propofol injection in the LR 0.3, LR 0.5 and LR 1.0 groups (37.5%, 12.5%, and 10%, respectively, P < 0.05) was significantly lower than that in the LS group (65%). The incidence of moderate pain disappeared completely in the LR 0.3, LR 0.5 and LR 1.0 groups (0%) compared with that in the LS group (20%). The LR 0.5 and LR 1.0 groups showed significantly less frequent and intense pain than the LR 0.3. However, there was a similar incidence of injection pain in the LR 0.5 and LR 1.0 groups.
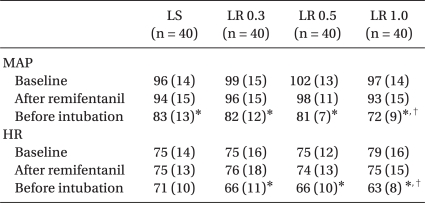
For all subjects, BIS score were above 90 before the microemulsion propofol injection, indicating adequate responses to questionnaires. The decrease in HR and MAP before intubation was statistically significant in all groups except HR in the LS group compared to the baseline value and in the LR 1.0 group compared to the LS group. However, the decrease of HR and MAP are of no clinical importance (Table 3). None of the patients suffered from desaturation or chest wall rigidity during the induction of anesthesia. There were no adverse effects observed at the injection site in any patient.
Discussion
Propofol-induced pain is a common problem and can be very distressing to the patient. It has been ranked by American anesthesiologists as the seventh most important drawback of current clinical anesthesiology [22].
Although the precise mechanism by which propofol induces pain at the time of injection has remained unclear, many factors that influence pain during propofol injection are known, including the speed of injection, speed of IV carrier fluid, and the buffering effect of blood [23,24]. Previous studies have shown that younger patients, patients with a peripheral IV site, female patients in general and female patients at the follicular phase of the menstrual cycle are more sensitive to pain on the injection of propofol [25,26]. In addition, it has been reported that the incidence and severity of pain during propofol injection was related to the formulation of propofol [8,27].
In this study, there was a significantly lower incidence and intensity of microemulsion propofol injection pain in the combination group than in the LS group (P < 0.05). The LR 0.5 and LR 1.0 groups showed significantly less frequent and intense pain than the LR 0.3 group (P < 0.05). There was a similar incidence of injection pain in the LR 0.5 and LR 1.0 groups.
The most popular method for reducing injection pain is to mix lidocaine with propofol. This technique is easy, fast, does not affect the physiochemical property of the drug and more importantly is associated with a clinically and statistically significant reduction in the incidence and severity of pain [13,23]. The mechanism of the analgesic effect of lidocaine remains unclear, but is generally considered to be by the inhibition of the kinnin cascade [23,28] or the dilutional effect on propofol [29].
Pretreatment with remifentanil has been reported to reduce the incidence and severity of pain during propofol injection [15,16]. Similar to other opioids, the action site of remifentanil may either be central or peripheral. Previous studies have shown that intravenous opioids given as Bier's block before propofol injection failed to show analgesic efficacy [30,31]. In this study, the patients received remifentanil and then 90 seconds later they received the microemulsion propofol injection. Thus, the mechanism of the analgesic effect of remifentanil may be related mainly to a central effect.
However, some patients do not respond well to lidocaine mixed with propofol and some patients continue to complain even with lidocaine administration. Moreover, the incidence of a painful injection of microemulsion propofol mixed with lidocaine 40 mg in our study was ~65%. A previous study showed that remifentanil was effective in preventing propofol injection pain, and should be used at a dose of at least 0.02 mg for this purpose [15]. However, in a previous study, an intravenous remifentanil 0.5 µg/kg pretreatment was not effective in alleviating pain associated with a microemulsion propofol injection and the incidence of a painful injection was 90% [20]. As a result, this incidence is unacceptable, which lead us to search for a new method. Recent studies show that combination therapy using different analgesic modalities can reduce the incidence and severity of propofol injection pain [17-19]. Also, recent studies revealed that a combination of opioids and lidocaine can reduce the incidence and severity of propofol injection pain compared to each drug used alone in adults [17,32]. In our study, the incidence of pain from the microemulsion propofol injection in the LR 0.3, LR 0.5 and LR 1.0 groups (37.5%, 12.5%, and 10%, respectively) was significantly lower than that in the LS group (65%). A previous study show that the combination of pretreatment of remifentanil (0.35 µg/kg/min) and a premixture of lidocaine with propofol (mixture of propofol 1% and lidocaine 1% in a 10 : 1 ratio) is more effective in reducing the incidence of pain on injection of propofol than either treatment alone [32]. Also, in this study, the combination of pretreatment of remifentanil and premixture of lidocaine with microemulsion propofol was more effective in a dose-dependent manner. The mechanism of action involved has not been identified, but it is possible that remifentanil enhances the analgesic efficacy of the lidocaine premixture. Further study elucidating the mechanism of this effect is therefore required.
Although, the decrease in HR and MAP before intubation was statistically significant in all groups except HR in the LS group compared to the baseline value, and in the LR 1.0 group compared to the LS group, the decrease of HR and MAP were of no clinical importance (Table 3). None of the patients suffered from desaturation, apnea and chest wall rigidity during the induction of anesthesia. For all subjects, BIS score were above 90, indicating adequate responses to questionnaires. There were no adverse effects at the injection site in any patient.
These findings should be considered within the context of the limitation of this study. First, we did not use higher doses of remifentanil. Higher doses of remifentanil would possibly produce further reductions in propofol injection pain. This will be of clinical benefit if it is not associated with an increase in the incidence of complications. Second, a non-treated control group was not included in this study. However, because microemulsion propofol produces more frequent and severe pain upon injection than lipid emulsion propofol, including a non-treated arm would not have been ethical.
In conclusion, a combination of pretreatment of remifentanil with premixture of lidocaine with microemulsion propofol was more effective in reducing the incidence of pain on injection of microemulsion propofol than just a premixture of lidocaine with microemulsion propofol alone. The combination of pretreatment of remifentanil 0.5 µg/kg and premixure of lidocaine 40 mg had a similar analgesic effect compared to the combination of pretreatment of remifentanil 1.0 µg/kg and premixure of lidocaine.
 XML Download
XML Download