

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Growth differentiation factor-15 (GDF-15), also known as macrophage inhibiting cytokine-1 and nonsteroidal anti-inflammatory drug-activated gene-1 [1], is synthesized as a propeptide and undergoes cleavage of its N-terminus to generate an active 25-kD disulfide-linked dimeric active protein. Normally, GDF-15 is highly expressed in the prostate and placenta, as well as in the heart, pancreas, liver, kidney, and colon [23]. GDF-15 is a member of the transforming growth factor-β (TGF-β) superfamily and is rapidly expressed in response to cytokines and growth factors, such as interleukin 1β (IL-1β), tumor necrosis factor-α (TNF-α), angiotensin II, macrophage colony stimulating factor, and TGF-β [24]. High levels of GDF-15 are associated with both cardiovascular and noncardiovascular mortality [5]. GDF-15 levels are independently positively correlated with smoking, diabetes, cardiovascular disorders, renal dysfunction and markers of inflammation, such as C-reactive protein (CRP). High GDF-15 levels are also a strong predictor of overall mortality in healthy subjects without previous cardiovascular disease or cancer [6].
Statins not only lower blood cholesterol levels by inhibiting 3-hydroxy-3-methylglutaryl coenzyme A reductase but also have anti-inflammatory effects. As a modulator of several inflammatory mechanisms [7], statins can improve cardiac outcomes [8910]. In the pravastatin inflammation/CRP evaluation (PRINCE) trial, the serum CRP level was significantly decreased independent of low density lipoprotein cholesterol (LDL-C) changes after treatment with pravastatin (40 mg/day for 24 weeks) in patients with coronary artery disease [11]. In another trial, statin treatment reduced inflammation-associated markers, such as CRP, TNF-α, IL-1, IL-6, and soluble intercellular adhesion molecule-1 in hypercholesterolemic patients [1213].
The role of inflammation in the pathogenesis of type 2 diabetes and associated complications is well established [14]. Recent studies regarding the treatment of type 2 diabetes focused on delaying disease progression using anti-inflammatory drugs and not only on lowering glucose [15]. Recently, several studies showed GDF-15 to be a stress-responsive cytokine that is increased in obesity, prediabetes and type 2 diabetic patients [16171819] and is a predictive and prognostic factor for cardiovascular disease and diabetes [2021]. However, reports regarding the effect of statins on GDF-15 levels are lacking, although statins are commonly prescribed to patients with cardiovascular risk factors. Statins decrease the level of LDL-C and the risk of cardiovascular disease. This study was performed to verify the effectiveness of GDF-15 as a prognostic factor for cardiovascular disease in diabetes and as a diagnostic marker of diabetes and cardiovascular disease by observing the change in GDF-15 levels as LDL-C levels decrease in response to statin therapy.
METHODS
Study design
Fifty-nine type 2 diabetic patients with LDL-C levels ≥100 mg/dL that visited the Endocrinology Department of Chungnam National University Hospital from February 2013 to March 2014 were enrolled in this study. Exclusion criteria were a history of lipid lowering medication within 4 weeks (including the screening period), hypersensitivity or resistance to atorvastatin, elevated aspartate transaminase (AST) or alanine transaminase (ALT; more than two times the normal highest value), elevated creatinine (Cr ≥1.5 mg/dL), elevated creatine kinase (more than two times the normal highest value). Patients with acute infectious disease and a history of acute myocardial infarctions within 6 months were also excluded.
Of the 59 participants, 50 were included in the final analysis and 9 were excluded due to the cancellation of acceptance (n=3), screening failure (n=3), or poor compliance (n=3). The patients were randomly divided into two groups based on the amount of atorvastatin prescribed as the 10 mg/day (n=23) and 40 mg/day atorvastatin groups (n=27). Plasma samples were obtained from all patients for the measurement of biochemical markers at baseline and after 8 weeks of treatment (Fig. 1). Side effects due to atorvastatin were not observed during the study.
Biochemical data
The blood samples were collected using ethylenediaminetetraacetic acid tubes in the morning after an overnight fast of more than 8 hours, and the lipid profiles (high density lipoprotein cholesterol [HDL-C], LDL-C, total cholesterol [TC], and triglycerides [TGs]) were measured using a blood chemistry analyzer (Hitachi 747; Hitachi, Tokyo, Japan). CRP was measured using the photometric latex agglutination method (TBA-2000FR; Toshiba, Tokyo, Japan). Insulin was quantified using an immunoradiometric assay kit (DIAsource INS-IRMA Kit; DIAsource, Louvain-la-Neuve, Belgium). Glycosylated hemoglobin (HbA1c) was measured using high-performance liquid chromatography (BioRad, Hercules, CA, USA). Homeostasis model assessment-estimated insulin resistance (HOMA-IR) was calculated as the fasting serum insulin (µU/mL)×fasting plasma glucose (mmol/L)/22.5. The fasting serum GDF-15 level was measured using a quantitative sandwich enzyme immunoassay technique with an enzyme-linked immunosorbent assay (ELISA; R&D systems, Minneapolis, MN, USA; and Quantikine ELISA, Human GDF-15, catalog number: DGD150).
Statistical analyses
All parameter values were calculated as the mean±standard deviations. A P<0.05 was considered statistically significant. Chi-square and Mann-Whitney U tests were used to compare the clinical characteristics and biochemical data between the two groups. The Wilcoxon signed-rank test was used to compare the biochemical data at baseline and after 8 weeks of treatment. The difference in biochemical data was compared before and after 8 weeks of treatment using the Mann-Whitney U test. To analyze the strength of the relationship between the differences in GDF-15 and biochemical data, Pearson correlation coefficients were used. Differences in the evaluated variables between the responder group (GDF-15 decreased after treatment) and nonresponder group (GDF-15 not decreased after treatment) were compared using the Mann-Whitney U test. Statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The clinical characteristics of the study population are shown in Table 1. The mean age was not significantly different between the 10 mg atorvastatin (56.0±11.4 years) and 40 mg atorvastatin groups (55.2±13.3 years). Other variables, including gender, weight, height, blood pressure, and pulse rate were not significantly different between the two groups (Table 1).
Multiple variables were compared between the two groups at baseline and after 8 weeks of treatment. The TC, LDL-C, and TGs were significantly decreased in both groups after 8 weeks of treatment. However, the changes in creatine phosphokinase, ALT, AST, insulin, C-peptide, HbA1c, glucose, HDL-C, and HOMA-IR index were not significant. Among the 50 participants, high-sensitivity C-reactive protein (hsCRP) was measured in 31 subjects (16 in the 10 mg atorvastatin group and 15 in the 40 mg atorvastatin group). A significant reduction in hsCRP was found in the 10 mg atorvastatin group (P=0.020) and 40 mg atorvastatin group (P=0.018). However, GDF-15 was not significantly changed in either group (Table 2).
Comparison of the two groups showed that none of the variables were significantly different compared to the baseline levels, except LDL-C (82.7±18.8 mg/dL vs. 68.0±22.7 mg/dL, P=0.006) and TC (148.2±24.1 mg/dL vs. 132.3±26.2 mg/dL, P=0.023), which were lower in the 40 mg group than the 10 mg atorvastatin group after treatment. Other variables were not significantly different between the two groups after treatment (Table 3).
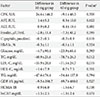
After analyzing the changes in numerous clinical parameters for each group, the differences in TC (P=0.012) and LDL-C (P=0.019) were significantly greater in the 40 mg atorvastatin group. The degree of difference for all other factors was not significantly different (Table 4).
The extent of change in the GDF-15 levels and other diverse clinical factors after treatment was not statistically significantly correlated (Table 5).
Cases with reduced GDF-15 levels after treatment were classified as 'responders' and those without reduced levels as 'non-responders,' and the clinical characteristics were then analyzed in each group. The responder group had more patients with hypertension (P=0.026), whereas the other factors were not significant (Table 6).
DISCUSSION
This study investigated the effect of treatment with atorvastatin on metabolic parameters and GDF-15 levels in type 2 diabetic patients. After treatment with atorvastatin, the levels of TC, LDL-C, and TGs were reduced, with greater reductions in the 40 mg compared to the 10 mg atorvastatin group, as expected. Additionally, hsCRP was reduced after treatment with atorvastatin; however, GDF-15 was not significantly changed in either group.
Comparison of the responder group, which showed decreased GDF-15 levels after statin therapy, and the non-responder group, which showed no decreased GDF-15, indicated that hypertension was only the significant common factor in the responder group. Other factors showed no significant difference between the two groups. In general, the GDF-15 level is increased in patients with hypertension, and Xu et al. [22] reported a positive correlation between GDF-15 and left ventricular hypertrophy, norepinephrine, and brain natriuretic peptide levels. Chen et al. [23] reported that the GDF-15 level was elevated in heart tissue based on a mouse model study of myocardial infarction after olmesartan treatment. In this study, there were 16 patients with hypertension, and 13 of 16 were treated with angiotensin receptor blockers or angiotensin converting enzyme inhibitors. These treatments may influence the baseline GDF-15 levels; however, because the type or dosage of these medications was not changed during the study, the effect was predicted to be insignificant.
The expression of GDF-15 is increased by high glucose or obesity [116172425], and high glucose induced GDF-15 expression is reactive oxygen species (ROS)- and p53-dependent [1]. High levels of GDF-15 indicate endothelial dysfunction and increase the risk of metabolic dysfunction, inflammation, vascular injury and accompanying cardiovascular complications [17]. Additionally, recent studies found that GDF-15 is a useful marker for the diagnosis of chronic inflammatory diseases, including prediabetes, diabetes, and acute coronary syndrome, cancer, chronic kidney diseases associated with oxidative stress, inflammation and endothelial dysfunction [262728293031]. However, reports on drugs affecting GDF-15 expression other than nonsteroidal anti-inflammatory drugs, which increase GDF-15 expression, are lacking [32]. Several studies analyzed the correlation between statins and GDF-15; however, the results were inconsistent. The pravastatin or atorvastatin evaluation and infection therapy-thrombolysis in myocardial infarction (PROVE-IT-TIMI) trial compared the mortality rates between intensive versus moderate statin therapy groups in acute coronary syndrome patients, and no significant change in GDF-15 after treatment with statins for 4 months was observed, which is consistent with our study results [33]. Conversely, another study evaluating the efficacy of GDF-15 for screening patients with heart failure showed that GDF-15 was lower in patients treated with statins due to a reduction in vascular inflammation but did not show changes of GDF-15 according to treatment with a statin [34].
Statins effectively modulate oxidative stress by reducing the generation of ROS [3536]. In an animal allograft model of atherosclerosis, statins inhibited the infiltration of inflammatory cells into the arterial wall by reducing the expression of chemokines, such as monocyte chemoattractant protein-1 [37]. Because oxidative stress and proinflammatory cytokines induce the expression of GDF-15 in macrophages, the authors hypothesized a negative correlation between statins and GDF-15 expression. However, in previous studies and our study, statin treatment did not affect GDF-15 levels. The short-term 4-month treatment period in our study and other previous studies, or the insufficient amount of atorvastatin (10 and 40 mg) may not cause any significant correlation between the two factors. In an apolipoprotein E-deficient mouse model, 10 g/kg/day atorvastatin significantly reduced macrophage infiltration in atherosclerotic plaques and the number of vulnerable plaques independently of a reduction in TC levels, and this treatment reduced chemokines and inflammatory markers, such as CRP and TNF-α [38]. Based on our study results, the dose of statins used was possibly insufficient, and further studies on the effect of high-dose statins on GDF-15 levels are needed. In another study, the effect of lowering the acute coronary event risk using statins was only significant in patients with low LDL-C levels [12]. However, because our study included patients with LDL-C over 100 mg/dL, these factors may have affected the results.
This study had several limitations, including insufficient dosage, duration of statin treatment and a small patient cohort. Although selection bias may have occurred due to a small study population, such bias was minimized through randomized control. Further studies are necessary to overcome such drawbacks.
In summary, treatment with 10 and 40 mg atorvastatin for 8 weeks reduced TC, LDL-C, and TG levels due to its lipid lowering effects and may affect inflammatory modulation by lowering hsCRP. However, atorvastatin had no significant effect on GDF-15 levels. Based on these results, we expect GDF-15 to be useful for the diagnosis of diabetes and acute coronary syndrome even when the patient is administered standard doses of statins.






 XML Download
XML Download