

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetic peripheral neuropathy (DPN) is suspected when diabetic patients complain of symptoms and/or show signs of peripheral nerve dysfunction after exclusion of other etiology [1]. This common complication of diabetes typically involve sensory nerves, motor nerves, and autonomic nerves, and often results in foot ulcers [2]. DPN can lead to socio-economic problems as well as psychological and physiological disorders [2]. Diagnosis and treatments are based on the medical history and results of a physical examination of patients with DPN [3]. The most widely used clinical nerve function examinations are the monofilament test [4], the vibration sensory test [5], and the ankle reflex test. Diagnostic sensitivity can reach up to 87% when more than two of the nerve function examinations are performed and other causes of neuropathy have been ruled out based on typical symptoms of DPN (careful with paresthesia) [1,6].
Pulse wave velocity (PWV) reflects arterial stiffness [7]. The oscillometric method, which is a simple non-invasive method, can be used to measure brachial-ankle pulse wave velocity (baPWV) [8], and in turn, baPWV can be used to detect vascular damage [9,10]. BaPWV reflects the condition of the aorta and peripheral arteries because it is affected by vasomotor reflexes, it is thought to have a greater association with microangiopathic conditions and diabetes complications than aortic pulse wave velocity [11]. Previous reports indicated that baPWV is an independent predictor of cardiovascular disease [12, 13], and its use as a clinical indicator is being reviewed.
Aso et al. [11] reported that baPWV was not only directly related to albuminuria, autonomic neuropathy, and retinopathy, but also peripheral neuropathy. Yokoyama et al. [14] reported that pulse wave velocity, retinopathy, age, and glycated hemoglobin are independent risk factors in DPN and the associated autonomic neuropathy. This study used a retrospective analysis to investigate DPN in type 2 diabetes patients and the association between baPWV and nerve function tests.
METHODS
This study received the approval of the clinical ethics committee (BSM 2011-04). Brachial pulse wave velocity was measured in type 2 diabetes patients in an outpatient clinic and in those admitted to the study hospital between January 2008 and August 2009. Total symptom scores and sensory function tests for DPN were retrospectively analyzed in 738 patients over 30 years old [6,15]. A total of 46 cases were excluded based on the following criteria: neuropathy caused by other etiology, severe heart failure, dialysis with chronic renal failure, cardiovascular disease, advanced cirrhosis, tumors, mental illness, thyroid disease, vitamin B12 deficiency, or an ankle brachial pressure index (ABI) on one side of 0.9 or lower. Gender, age, duration of diabetes, and medical history of all patients were noted. Resting blood pressure and pulse pressure were measured after patients rested in the supine position for 5 minutes. Height, weight, and waist circumferences were also measured. Body mass index (BMI) was measured by dividing body mass (kg) by height in meters squared (m2).
Participants were surveyed regarding alcohol consumption and smoking. Participants were considered to be drinkers if they consumed more than 20 g of alcohol per day. One serving of soju (180 mL) contains 45 g of alcohol, one serving of makgeolli (Korean rice wine) (1,800 mL) contains 144 g alcohol, and one bottle of beer (640 mL) contains 25.6 g of alcohol. Patients were surveyed to determine if they were receiving insulin therapy or taking thiazolidinedione, statins, antiplatelet agents, β-blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, α-lipoic acid, γ-linolenic acid, tricyclinc antidepressants, pregabalin, or gabapentin. Blood samples were collected after participants fasted for at least 8 hours. Total cholesterol, triglycerides, high density lipoprotein cholesterol, low density lipoprotein cholesterol, fasting blood glucose, fasting insulin, glycated hemoglobin, high sensitivity C-reactive protein (hs-CRP), aspartate aminotransferase, alanine aminotransferase, microalbuminuria, and gamma-glutamyltranspeptidase were measured from collected samples. BaPWV was calculated automatically using an automatic waveform analyzer (VP-1000; Colin, Komaki, Japan) [16] by dividing brachial-ankle distance (L=0.5934×height [cm]+14.4014) by the pulse wave time interval between the brachial region and ankle (ΔT) in patients who were stabilized in the supine position for 5 minutes.
Left and right baPWVs were measured, and the largest value was defined as the maximum baPWV (max-baPWV). The total symptom score was based on the severity and frequency of pain, burning, paresthesia, and numbness [15]. Symptom frequency was categorized as absent, seldom (from 2 to 3 times per week or less than once per day), often (1 to 2 times per day or 7 to 14 times per week), and constant (most of the day, or over 3 times per day every day). Severity was based on a visual analog scale. The levels were scored and separated into mild (does not interfere with everyday life), moderate (affects daily life, but does not affect sleep), and severe (interferes with sleep). Symptom scores were summed, and the total symptom scores calculated ranged from 0 to 14.64 (Table 1) [15]. A monofilament examination, ankle reflex test, and vibration test were performed to evaluate sensory function. When performing the monofilament test, patients lay down and closed their eyes. Ten-gram monofilaments were pressed into 10 points on the top and bottom of patients' feet until the monofilament began to bend. Patients were evaluated for sensation on the points, and if patients had sensation in fewer than seven points, then they were identified as having abnormal test.
To test ankle reflexes, patients lay down with their legs bent and their knees rotated externally. The researcher placed the patient's feet in a position of dorsiflexion and then tapped the Achilles tendon. Patients with a low or hyperactive response were determined to a abnormality in the test.
For the vibration sensory test, the oscillator was set at 128 Hz. Patients notified when they could not feel a vibration at the point (the first metatarso-phalangeal joint) where the toes were extended, and then investigator felt the vibration and measured time when the feeling had disappeared. The time difference ≥10 seconds between the investigator and the patient, patients were determined as an abnormality in the test.
When patients had a total symptom score of at least two and had abnormal sensory function tests, they were defined with probable DPN.
Statistical analyses were performed using SPSS for Windows version 14.0 (SPSS Inc., Chicago, IL, USA). Baseline characteristics were expressed as mean±standard deviation, and variables that were not normally distributed were expressed as median and interquartile values. Independent t-tests or chi-square tests were used to determine differences between the two groups. If the chi-squared tests indicated, Cochran and Mantel-Haenszel statistics were used to compensate confounding variables. Additionally, when baPWV could be used to predict DPN, a univariate logistic regression analysis, multivariate logistic regression analysis, odds ratios, and confidence interval (CI) for each risk factor were presented. A P value less than 0.05 was considered statistically significant.
RESULTS
There were a total of 692 participants in this study. The participants were divided into the baPWV ≥1,600 cm/sec group (n=356) and the <1,600 cm/sec group (n=336). The characteristics of each group are summarized in Table 2.
There was a greater proportion of females in the ≥1,600 cm/sec group compared to the <1,600 cm/sec group (62.0% vs. 51.5%, P<0.01). The mean age of patients was higher (62.0±9.5 vs. 51.5±9.6, P<0.01), and the duration of diabetes was longer (8.5±6.9 vs. 7.3±5.4, P<0.01) in the ≥1,600 cm/sec group. Additionally, systolic blood pressure (146.5±17.9 mm Hg vs. 126.2±12.0 mm Hg, P<0.01), diastolic blood pressure (84.5±10.5 mm Hg vs. 77.5±8.5 mm Hg, P<0.01), pulse pressure (62.0±13.3 mm Hg vs. 48.7±8.7 mm Hg, P<0.01), and glycated hemoglobin (7.7±1.7% vs. 7.3±1.5%, P<0.01) were higher in the ≥1,600 cm/sec group, and a greater proportion of this group used lipid lowering drugs (66.9% vs. 58.2%, P=0.019) when compared to the <1,600 cm/sec group. There was no significant difference in the percent of individual neuropathy treatment drugs between the ≥1,600 cm/sec group and the <1,600 cm/sec group, but there was a significant difference in the percent of the total neuropathy treatment drugs (56.2% vs. 47.3%, P<0.020) between the groups. Thus, lipid levels, fasting blood glucose, fasting insulin, and microalbuminuria were not significantly different between the ≥1,600 cm/sec group and the <1,600 cm/sec group.
This study also evaluated the differences between the patients with DPN (116 patients) and the patients without DPN (576 patients) (Table 3).
There were more women in the patients with DPN compared to the patients without DPN (66.4% vs. 52.1%, P<0.01), and the patients with DPN were older (59.6±10.7 years vs. 56.4±10.8 years, P<0.01), and had a higher systolic blood pressure (141.6±22.6 mm Hg vs. 135.6±17.2 mm Hg, P<0.01), and pulse pressure (59.4±13.4 mm Hg vs. 54.8±12.9 mm Hg, P<0.01) than the patients without DPN. There was a significant difference in the percent of γ-linolenic acid (37.0% vs. 24.0%, P<0.01), one of the individual neuropathy treatment drugs, between the patients with/without DPN. The proportion of total neuropathy treatment drugs prescribed (67.2% vs. 48.8%, P<0.01) was significantly higher in the patients with DPN.
The max-baPWV (1,790±398.3 cm/sec vs. 1,650.4±350.5 cm/sec, P<0.01) and the percent of baPWV ≥1,600 cm/sec were significantly higher (61.2% vs. 49.5%, P=0.020) in the patients with DPN compare to the patients without DPN.
Univariate analysis and multivariate logistic regression analyses of risk factors for DPN such as age, blood pressure, gender, and baPWV were performed after conversion into binary variables, and then odds ratios for each variable and CIs were calculated (Table 4).
The odds ratio of the baPWV ≥1,600 cm/sec was 1.611 (95% CI, 1.072 to 2.422; P=0.021) and the odds ratio in females was 1.816 (95% CI, 1.195 to 2,760; P=0.005) in the univariate analysis, which were both significantly higher than the control groups. However, the results of a multivariate logistic regression analysis showed that female was independent risk factor of DPN.
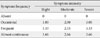
When the associations among baPWV and symptoms or signs of DPN were evaluated, paresthesia and numbness in baPWV ≥1,600 cm/sec group was higher than <1,600 cm/sec group (10.1% vs. 5.7%, P=0.035; 13.5% vs. 6.9%, P=0.006, respectively) (Table 5). There was no significant difference in pain and burning. The monofilament test abnormality showed that the ≥1,600 cm/sec group (14.9%) was significantly higher than the <1,600 cm/sec group (P<0.001). There was no significant difference in the vibration sensation and ankle reflex test between the two groups. Cases in which the total symptom score was 2 points or more, or the monofilament test abnormality, were significantly higher in the ≥1,600 cm/sec group (41.3%) compared to the <1,600 cm/sec group (31.6%) (P<0.01). When Cochran and Mantel-Haenszel statistical methods were used, after adjusting for age, numbness (P=0.026) and the monofilament test abnormality (P=0.009) were still significant.
DISCUSSION
The most common form of DPN is distal symmetry polyneuropathy (DSPN) [17]. Toronto Diabetic Neuropathy Expert Group proposed definitions of minimal criteria for DSPN [18].
The presence of an abnormality of nerve conduction was proposed to be the standard for confirmed diagnosis of DSPN [18]. However, the main pathological findings for early stage DPN are small nerve fiber damage [19,20], and this stage may not appear abnormality of nerve conduction reflected the function of large nerve fibers [21,22]. If nerve coduction is normal, a validated measure of small fiber neuropathy may be used for confirmed diagnosis of DSPN [18]. In this study, nerve conduction tests and small nerve dysfunction tests were not performed, so diagnosis could not be performed. Cases where the total symptom score is ≥2 and abnormal sensory functions are observed can be defined as probable DSPN.
Arterial pulse wave velocity reflects the stiffness of arteries, and is also an indicator of atherosclerosis [23]. By measuring baPWV, blood pressure and pulse wave velocity can be easily measured. The cutoff point of the baPWV for the prediction of cardiovascular disease based is varied, and a standard value has not been established. Kim and Kim [24] studied the relationship between baPWV and the risk of cardiovascular disease through a health screening of study subjects. baPWV ≥1,600 cm/sec was a independent risk factor for cardiovascular disease defined with the systemic coronary risk evaluation (SCORE) risk score [24]. Kim et al. [25] proposed that the cut-off point for the baPWV in type 2 diabetes patients with cardiovascular disease was 1,635 cm/sec (sensitivity 73%, specificity 75%). In our study, a receiver operating characteristic curve was used for analysis, but significant cutoff values of baPWV could not be obtained. So the cutoff value was set at 1,600 cm/sec based on the previously mentioned study.
When the variables were compared between the patients with/without DPN, patients with DPN had higher baPWV and were more likely to have baPWV ≥1,600 cm/sec. This explains the association between baPWV and DPN. In a univariate analysis of the risk factors for DPN, the odds ratio was 1.611 (95% CI, 1.072 to 2.422; P=0.021) in cases where baPWV was ≥1,600 cm/sec, which is a meaningful risk factor for DPN. A multivariate logistic regression analysis was performed to adjust for confounding variables and the adjusted odds ratio was 1.623 (95% CI, 0.975 to 2.701; P=0.062), which indicates that a baPWV ≥1,600 cm/sec was not an independent risk factor. However, even though the P value was greater than 0.05, the 95% CI was 0.975 to 2.701; therefore, as a precaution, it was suspected that a baPWV ≥1,600 cm/sec is a risk factor.
The primary factors affecting baPWV are age, systolic blood pressure, and gender [12]. In a study on type 2 diabetes patients, baPWV was significantly correlated with blood pressure, pulse pressure, age, waist circumference, and duration of diabetes [26]. In our study, when the ≥1,600 cm/sec group and the <1,600 cm/sec group were compared, gender, age, duration of diabetes, height, weight, waist circumference, systolic blood pressure, diastolic blood pressure, pulse pressure, and glycated hemoglobin were significantly different between the groups. Lipid levels were similar in the groups. These were likely caused by the different effects of each atherosclerosis risk factor on PWV. In other words, age and blood pressure are independent factors that have a powerful effect on PWV, whereas total cholesterol and low density lipoprotein cholesterol have a minor effect on PWV [13,27]. Either PWV has a greater association with sclerosis of the blood vessels [28], or lipid metabolism has a greater association with atherosclerosis. Additionally, the increased prescription rate of lipid lowering drugs is thought to have a partial effect. Angiotensin II receptor blockers and antiplatelet agents were relatively widely prescribed for increases in arterial stiffness. Use of lipid lowering drugs, angiotensin II receptor blockers, and antiplatelet agents have been reported to lower hs-CRP [29,30], and it is estimated that there is no significant difference in hs-CRP between the two groups.
Antioxidant α-lipoic acid reduces oxidative stress in the pathogenesis of DPN and is effective in improving symptoms and in preventing neurovascular damage [31-33]. The total of neuropathy treatment drugs was higher in the DPN group and baPWV ≥1,600 cm/sec group, and there was no difference in the prescription of individual neuropathy treatment drugs in these groups. In cases where there are symptoms but there are no signs of early stage DPN, neuropathy treatment drugs may be used for prevention or to improve symptoms. This study is limited because it is a cross-sectional study, and patients may have experienced improved symptoms due to drugs taken prior to assessment, or as a result of being placed in the group without DPN. When comparing nerve fibers based on size, large nerve fibers transmit the sensation of light pressure and vibration, and small nerve fibers transmit the sensation of pain and temperature [34]. After DPN causes initial small nerve fiber damage, large nerve fibers become damaged, and damage to large nerve fibers is less common [19,20]. Typically, at the initial stages of the disease, pain and abnormal sensations occur. Afterwards, sensation is lost, numbness occurs and pain and burning sensation can improve [35]. Monofilament tests are useful in measuring and detecting sensations of light pressure in large nerve fibers [36], and are inexpensive, easy to perform, and highly reproducible [37]. However, vibration sensory tests and ankle reflex tests are limited in their reproducibility. In this study, there was no increase in pain and burning sensations in baPWV ≥1,600 cm/sec group; however, there was a higher percent of numbness.
Among nerve function tests, monofilament tests showed a higher percent of abnormalities in the ≥1,600 cm/sec group compared to the <1,600 cm/sec group. Even after adjusting for age, the percent of the monofilament test abnormalities was significantly high. There were many patients in the ≥1,600 cm/sec group who showed relatively late stage symptoms of numbness and monofilament test abnormalities that reflected damage to large nerve fibers, which suggests that there is a correlation between baPWV and relatively advanced DPN.
There are several other limitations to this study. Nerve conduction tests were not performed, so the diagnosis of DPN was used as clinical criteria. In order to confirm diagnosis, the Toronto Diabetic Neuropathy Expert Group as well as Feldman et al. [38] claim that the Michigan Diabetes Neuropathy Score (MDNS) and a nerve conduction test (or validate measure of small fiber neuropathy) must be performed [18,37]. However, in this study, sufficient data of MDNS and nerve conduction test could not be acquired due to the limitations of retrospective studies. In addition, the baPWV need to do regression against neuropathy score. Thus, further research is required. In conclusion, increased baPWV was correlated with DPN in patients with type 2 diabetes.




 XML Download
XML Download