

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The left ventricular (LV) to right atrial (RA) shunt is an uncommon congenital or acquired heart disorder known as Gerbode defect (GD).1) The development of advanced cardiovascular imaging and percutaneous therapeutic options have had an important role in the diagnosis and management of the GD. In particular, the use of 3D transesophageal echocardiography (TEE) is at the forefront of diagnosis, decision making and catheter based treatment guidance.
Case
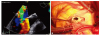
A 55-year-old woman presented with worsening dyspnea over the past 12 months. She had no medical or surgical history. Cardiovascular risk factors associated were arterial hypertension, hypercholesterolemia, former smoking history and obesity (body mass index 32.9 kg/m2). The physical examination was normal, except for a 3/6 systolic murmur audible at the apex and along the left sternal border. The electrocardiogram was also normal. Chest X-ray showed situs solitus, levocardia, mildly increased cardiothoracic index, and pulmonary plethora. TTE revealed severe mitral regurgitation (MR) due to a mitral valve structural abnormality. A linear structure was present in the left ventricle outflow tract (LVOT) connecting the basal interventricular septum with the tip of the anterior mitral leaflet, restricting the mitral valve motion and causing severe MR. There was no evidence of LVOT obstruction. Both LV volumes and ejection fraction were normal, with no wall motion abnormalities. An abnormal high velocity systolic jet was visualized in the RA (Fig. 1A and Supplementary Video 1 in the online-only Data Supplement) with a peak velocity of 5.2 m/s (Fig. 1B). There were no indirect signs of pulmonary hypertension. Therefore, an abnormal communication between the LV and the RA was suspected. The TEE exam confirmed the LV to RA shunt above the septal leaflet of the tricuspid valve consistent with a Gerbode type defect (Fig. 1C, D and Supplementary Video 2 in the onlineonly Data Supplement). TEE also revealed a more detailed linear structure in the LVOT (Supplementary Video 3 in the online-only Data Supplement) connecting the basal interventricular septum with the tip of the anterior mitral leaflet, restricting the mitral valve motion and causing severe MR (Fig. 2A and Supplementary Video 4 in the online-only Data Supplement).
The preoperative coronary angiography revealed normal coronary arteries. No opacification of the RA during left ventriculography was observed, and the absence of pulmonary hypertension was confirmed at right heart catheterization. The patient underwent successful mitral valve replacement with a mechanical prosthesis and resection of abnormal LVOT chord, as well as repair of the Gerbode defect (covered with patch), with good outcome (Fig. 2B). At 6 months follow-up, the patient had a good clinical status, and the TTE examination showed a normally functioning mitral prosthesis with no residual LV to RA shunt.
Discussion
The first case of LV to RA shunt was described by Thurnan in 1838.2) Gerbode et al.3) collected the first series of five patients who underwent successful surgical correction of congenital LV to RA shunts in 1958. Classically, there have been two different types of GD based upon their relationship to the septal leaflet of the tricuspid valve: the supravalvular and the infravalvular. The infravalvular type is the most common, usually congenital, and is characterized by a perimembranous ventricular septal defect associated with cleft-shaped or perforation of tricuspid valve with an indirect LV to RA shunt. In the supravalvular type, communication is located in the atrioventricular portion of the membranous septum, producing a direct LV to RA shunt.4) The congenital etiology is the most common. Acquired cases have been associated with infective endocarditis, myocardial infarction, valvular replacement surgery, or radio frequency ablation of the atrioventricular node. No information about history of trauma, myocardial infarction or endocarditis could be elicited after careful questioning and examination. Considering also the morphologic abnormality of the mitral valve, the LV to RA shunt can be considered a congenital anomaly. Another peculiarity of the present case is the discovery of these congenital abnormalities in adulthood.
The high-velocity systolic Doppler flow signal in the RA may be misinterpreted as tricuspid regurgitant jet leading to the suspicion of pulmonary hypertension. Misdiagnosis can be prevented by careful evaluation of jet direction and by estimating the pulmonary pressure from the pulmonary regurgitation jet signal. In this case, there were no signs of right heart volume or pressure overload, and the velocity of the pulmonary regurgitant jet was low, suggesting normal pulmonary pressure (confirmed by catheterization).
Echocardiography is the mainstay in the diagnosis of the GD.5) Although TTE has a high sensitivity for the detection of LV to RA shunts, it is often difficult to diagnose the exact anatomic location and relationships of the shunts. It can also be difficult to distinguish with TTE the LV to RA shunt from a sinus of Valsalva rupture, endocardial cushion defect, ventricular septal defect or tricuspid regurgitation.6)7) A high velocity jet with an unclear origin detected in the RA requires additional imaging, including TEE, cardiac catheterization, or cardiac magnetic resonance for differential diagnosis.8) TEE can avoid diagnostic errors allowing to identify the trajectory and location of the communication, as well as its dimensions. In this setting, 3D echocardiography may also have an important role. 3D TEE is useful not only for the LV to RA shunt diagnosis, but also for the deciding the treatment plan. 3D TEE is an important imaging method for guiding the sizing and placement of percutaneous closure as well as surgical tactics.
In conclusion, we presented here a rare case of congenital Gerbode defect associated with severe mitral regurgitation due to a structural abnormality of the mitral valve apparatus, diagnosed in a 55 year-old patient. The case highlights the importance of a thorough examination interpreting the echocardiographic findings on a pathophysiological basis. It also underlines the complementary role of different imaging techniques with TEE, allowing the precise assessment of both structural and functional abnormalities in such a complex case. The imaging findings were confirmed during the surgical procedure, leading to good outcome.

 XML Download
XML Download