

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide, with 17.3 million deaths in 2008.1) Of these deaths, an estimated 7.3 million were due to coronary artery disease (CAD),1) and CAD has become a major public health problem involving high societal cost. These statistics highlight the importance of identifying risk and protective factors for CAD to promote better health for patients with CAD and the general population. Dyslipidemia, hypertension, smoking, and diabetes are well-established risk factors for CAD, yet they account for only two thirds of incidence of CAD.2)
Considerable emphasis has been placed on psychological factors as relevant risk factors for CAD, since growing evidence has suggested that many CAD patients experience high levels of anxiety, depression, or stress.3)4) Majority of studies suggested that psychological maladjustment, such as depression,5) anxiety,6) hostility,7) and work stress8) were important risk factors for the development of CAD. Recently, as advances in cardiac care and interventions improve health outcomes and life expectancy of patients with CAD, the importance of patients' overall quality of life on physical, mental, and social domains has been widely recognized.9) Researchers have begun to investigate quality of life in relation to cardiovascular health, and reported that people with CAD had poorer quality of life compared with the normal population.10) Additionally, impaired quality of life is associated with biological risk for CVD11) and increased future mortality.12) Perception of control, belief about one's capacity to affect and shape one's environment, have been recognized as important factors accounting for individual difference in psychological states among people with physical illness. Many studies have reported that control-enhancing strategies could be important protective factors.13) Primary control strategies refer to capacity to actively change ones' circumstance, while secondary control strategies are defined as compensatory strategies to cope with the unattainable goal.14) Both control strategies are associated with better medical outcomes and subjective well-being in the general population.14)15) However, little is known about control strategies among CAD patients.
Most of the research investigating contributions of psychological maladjustment to CAD has been carried out without paying attention to influence of quality of life or control strategies on CAD. Rarely has research examined multiple psychological factors simultaneously, such as psychological maladjustment, quality of life, and control strategies, hence the relative contributions of each psychological factor to development of CAD are still unclear. In Korea, only a handful of studies examining limited psychological factors have investigated the relationship between psychological factors and CAD.16) The purpose of current study was thus to assess levels of psychological maladjustment, such as anxiety, hostility, and work stress, health-related quality of life (HRQoL), and primary and secondary control strategy use in patients with acute coronary syndrome (ACS) in comparison with normal healthy subjects, and to identify psychological predictors of the development of ACS.
Subjects and Methods
Study design and subjects
The present study was designed as a cross-sectional research comparing ACS patients with normal healthy subjects. Eighty five patients with ACS (52.6±10.2 years, 17 women) and 63 healthy controls (48.7±6.7 years, 20 women) were recruited in the study between December 2011 and March 2013 in Ewha Womans University Mokdong Hospital. Cardiology clinic patients aged from 18 to 70 who met the diagnostic criteria for unstable angina (n=56) and acute myocardial infarction (AMI) (n=29) based on typical ischemic chest pain, electrocardiography findings, cardiac enzymes, echocardiography, coronary angiography, and cardiac CT angiography were included. The control group was healthy subjects drawn from the Health Promotion Center of the same institute. The control group had no clinical evidence and history of cardiovascular diseases, dyslipidemia, hypertension, diabetes, and other significant medical or surgical illness, and met the following criteria: 1) serum total cholesterol <220 mg/dL, 2) serum triglyceride <150 mg/dL, 3) serum glucose <110 mg/dL, and 4) systolic blood pressure <140 mm Hg and diastolic blood pressure <90 mm Hg. Blood samples after overnight fasting were collected. Within 2-3 weeks after being diagnosed, the ACS group was asked to complete questionnaires about their socio-demographic information, anxiety, hostility, work stress, HRQoL, and control strategies. Participants were informed about the purpose of the study, and a written informed consent was obtained. This study was approved by the Institutional Review Board of the Ewha Womans University Mokdong Hospital (No=ECT 12-01-10).
Assessment of anxiety
The Beck Anxiety Inventory (BAI) was designed to measure the degree of clinical anxiety.17) The BAI is composed of 21 items about symptoms of anxiety (e.g., 'unable to relax', 'fear of the worst happening', 'dizzy or lightheaded'). Participants were asked to rate their feelings about the symptom during the last week using a 4-point scale. Total score ranges from 0 to 63, and high score indicates high level of anxiety. Internal consistency (Cronbach's α) was 0.92 in the original study,17) and was 0.94 in the present study.
Assessment of hostility
The questionnaire to measure hostility was composed of 6 questions of the hostility scale derived from the Symptom Checklist-90-Revised (SCL-90-R) that has been widely used to assess psychopathological symptoms.18) Participants were asked to rate psycho-logical symptoms during the past 7 days (e.g., 'feeling easily annoyed or irritated', 'temper outbursts that you could not control', 'having urges to beat, injure, or harm someone') using a 5-point scale ranging from 0 (never) to 4 (very severe). Cronbach's α was 0.88 in the present study.
Assessment of work stress
Work stress was assessed by 14 questions of the Job Content Qu-estionnaire (JCQ) which measures 2 dimensions of Karasek's job strain model: the decision latitude (e.g., 'my job requires that I learn new things', 'my job requires me to be creative', 'my job allows me to make a lot of decisions on my own') and psychological job demand (e.g., 'my job requires working very fast', 'my job requires working very hard', 'I am not asked to do an excessive amount of work').19) Four types of job were classified from combinations of the decision latitude and psychological job demand: 'active job' (high demand and high decision latitude), 'high strain job' (high demand and low decision latitude), 'low strain job' (low demand and high decision latitude), and 'passive job' (low demand and low decision latitude). This model proposes that people with high psychological job demand and low decision latitude at work are likely to experience high level of stress at work. Difference of work stress between the ACS group and control group was analyzed by comparing proportions of high strain group. The decision latitude was scored from 24 to 96, and the psychological job demand was scored from 12 to 48. Cronbach's α for the decision latitude and job demand subscales were 0.81 and 0.63, respectively, in a previous study,19) and were 0.72 and 0.31, respectively, in the current study.
Assessment of health-related quality of life
The Medical Outcome Study Short Form 36 version 1 (SF-36) has been widely used to assess HRQoL in clinical research. This scale was originally designed to measure 8 components of health status: 1) physical functioning (PF, 10 items: e.g., 'Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports'; 'Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf'), 2) social functioning (SF, 2 items: e.g., 'During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbors, or groups?'), 3) role limitations due to physical problems (RP, 4 items: e.g., 'Cut down on the amount of time you spent on work or other activities as a result of your physical health', 'Accomplished less than you would like as a result of your physical health'), 4) role limitation due to emotional problems (RE, 3 items: 'Cut down on the amount of time you spent on work or other activities as a result of your emotional health', 'Accomplished less than you would like as a result of your emotional health'), 5) general mental health (MH, 5 items: e.g., 'Have you been a very nervous person?', 'Have you felt so down in the dumps that nothing could cheer you up?'), 6) vitality (VT, 4 items: e.g., 'Did you have a lot of energy?', 'Did you feel worn out?'), 7) bodily pain {BP, 2 items: e.g., 'How much bodily pain have you had during the past 4 weeks?', 'During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework) ?'}, 8) general health perceptions (GH, 5 items: e.g., 'I seem to get sick a little easier than other people', 'I am as healthy as anybody I know').20) These components represent two major dimensions of health: physical health and psychological well-being. Responses are scored from 0 to 100, and high score indicates better health on each component. Cronbach's α coefficients for the 8 scales ranged from 0.69 to 0.85 in the current study.
Assessment of control strategies
Control strategies were measured using a modified version of Wrosch, Heckhasuen and Lachma's primary and secondary control strategies scale.21) The modified control strategies scale consists of 21 items with a 5-point scale, and has 5 subscales: 1) persistence in goal striving (primary control: e.g., 'When things don't go according to my plans, my motto is, "Where there's a will, there's a way."', 'When faced with a bad situation, I do what I can do to change it for better'); 2) investment of effort and time (primary control: e.g., 'When I have a goal, I am willing to work hard at sharpening the skills in order to achieve it', 'When I really want something, I am able to work hard to achieve it'); 3) positive reappraisals (secondary control: e.g., 'I find I usually learn something meaningful from a difficult situation', 'When I am faced with a bad situation, it helps to find a different way of looking at things'); 4) lowering aspirations (secondary control: e.g., 'When my expectations are not being met, I lower my expectations', 'To avoid disappointments, I don't set my goals too high'); 5) downward comparison and self-protective attribution (secondary control: e.g., 'When something bad happens to me, I think of all the others who are much worse off than I am', 'When things don't work out for me, I tell myself that it was just bad luck'). Higher scores of each subscale indicate higher use of each strategy. Cronbach's α coefficients for the 5 subscales ranged from 0.57 to 0.84 in a previous study,21) and ranged from 0.49 to 0.85 in the current study.
Statistical analysis
Data were expressed as mean±standard deviation, and all analyses were conducted by Statistical Package for the Social Sciences (SPSS) version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows. An unpaired t-test and a chi-square test were performed to assess any significant difference in continuous and categorical variables, respectively, between the ACS group and control group. A univariate analysis of covariance (ANCOVA) was used to compare levels of anxiety and hostility between 2 groups after adjustment of age and gender. Participants were classified into 4 types of job, and difference of work stress between 2 groups was analyzed by a chi-square test. A multivariate ANCOVA was conducted to examine differences between 2 groups in level of HRQoL after adjustment of age and gender. The distribution of the participants' use of primary and secondary control strategies was divided into 4 groups by quartile value, respectively, and compared between 2 groups using a chi-square test.
A multivariate logistic regression analysis was performed to identify independent predictors of ACS after adjustment of age and gender. Several HRQoL subscales satisfying an F value >3.0 in the ANCOVA assay were classified into the physical or mental domain of HRQoL. The physical domain of HRQoL was calculated as an average of the GH, RP, and BP, and the mental domain of HRQoL was calculated as an average of the SF and VT. The primary control strategy was created by averaging the 2 primary control strategies subscales: 1) the persistence in goal achievement and 2) investment of effort and time. The secondary control strategy was the average of 3 secondary control strategies subscales: 1) the positive reappraisals, 2) lowering aspirations, and 3) downward comparison and self-protective attribution. Variables included in this analysis were as follows: the BAI, hostility scale of SCL-90, decision latitude, job demand, physical and mental domains of HRQoL, primary control strategy, and secondary control strategy. These variables were graded by quartile for the analysis. A p<0.05 was considered as statistically significant.
Results
Characteristics of study population
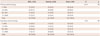
The general characteristics of ACS patients and healthy controls were presented in Table 1. Generally, the ACS group and control group differed significantly in age, gender, marital status, education, and income. Compared with the control group, the ACS group was older (52.6±10.2 years vs. 48.7±6.7 years, p<0.01), composed of more men (p<0.05), less likely to live with their partner (p<0.01), less educated (less than an undergraduate) (p<0.05), and had less income (p<0.001). However, the 2 groups were not different in having religion {p=not significant (NS)}.
Comparisons of psychological maladjustment
The levels of anxiety and hostility, assessed by the BAI and SCL-90-R, respectively, tended to be higher in the ACS group compared with the controls, but these differences, assessed by a univariate ANCOVA after adjustment of age and gender, did not reach statistical significance (Table 2). Four types of jobs to assess work stress, such as high strain, low strain, active, and passive jobs, were identified by the JCQ measuring 2 dimensions of Karasek's job strain model. There was no significant difference in the distribution of these 4 types of job analyzed by a chi-square test (p=NS) (Table 3).
Comparisons of health-related quality of life
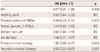
A multivariate ANCOVA was used to compare HRQoL between the ACS group and control group after controlling for age and gender. There were significant differences in HRQoL assessed by the SF-36 between 2 groups {F (8, 137)=5.507, p<0.001}. The ACS group had significantly lower scores on the GH (58.2±14.5 vs. 69.8±13.6, p<0.001) and BP (73.8±21.0 vs. 85.6±13.6, p<0.001) than the control group (Table 4). Additionally, the ACS group, compared with control group, had lower levels of the RP (80.2±20.7 vs. 85.3±17.3, p=0.06), SF (83.3±17.0 vs. 87.3±15.6, p=0.071), and VT (58.6±15.5 vs. 62.3±13.5, p=0.078) with borderline significance (Table 4). There was no significant difference in the PF, RE, and MH between 2 groups.
Comparisons of use of primary and secondary control strategies
Use of primary and secondary control strategies was graded by quartile values and compared between 2 groups using a chi-square test (Table 5). The ACS group tended to use primary control strategy more, although not statistically significant, with greater value at 50-75% (25.3% vs. 22.6%) and less value at 25-50% (24.1% vs. 29.0%) compared to the control group. On the other hand, the control group tended to use secondary control strategy more, although not statistically significant, with greater value at 75-100% (28.6% vs. 21.3%) and lower value at 25-50% (23.2% vs. 28.8%) compared to the ACS group.
Identification of independent predictors for acute coronary syndrome
A multivariate logistic regression analysis was conducted to identify independent predictors of ACS development after adjustment of age and gender. The multivariate logistic regression analysis sh-owed that the physical domain of HRQoL {odds ratio (OR): 0.40; 95% confidence interval (CI): 0.23 to 0.71, p=0.002}, primary control strategy (OR: 1.92; 95% CI: 1.09 to 3.37, p=0.024), and secondary control strategy (OR: 0.53; 95% CI: 0.33 to 0.87, p=0.012) were determined as independent predictors of ACS (Table 6).
Discussion
The present study was carried out to assess psychological well-being, ill-being, and control strategy factors in patients with ACS in comparison with normal healthy control subjects. Our data showed that ACS group, compared with the control group, had poor HRQoL, and that physical domain of HRQoL was determined as an independent predictor of ACS. Additionally, the ACS group tended to use primary control strategies more, while the control group tended to use secondary control strategies more. Although this tendency of control strategies was not significantly different between 2 groups by a univariate analysis, these control strategies were determined as significant independent predictors of ACS after adjustment of age and gender by multivariate logistic regression analysis. On the other hand, we could not find any significant difference between the ACS group and control group in levels of psychological maladjustment such as anxiety, hostility, and work stress.
Detrimental effects of psychological ill-being factors on CAD have been studied previously.8)22) On the other hand, a growing body of evidence showed protective effects of psychological well-being factors.10) Since the absence of ill-being does not necessarily mean well-being, assessment of well-being factors as well as ill-being factors is critical to assess integrated psychological status. HRQoL is a subjective outcome measure of overall well-being including physical, psychological, and social well-being and perceived health, and reflects the discrepancy between actual and desired function.10) The present study suggests that ACS patients had impaired quality of life significantly in the fields of GH and BP, and, with borderline significance, in the fields of role limitation due to physical problems, SF, and VT. The physical domain of HRQoL, calculated as an average of GH, role limitation due to physical problems, and BP, was determined as an independent predictor of ACS. However, we could not discern whether this relationship between HRQoL and ACS is cause or effect, since the present study was not designed as a prospective study. Impairment of quality of life in subjects with CAD has been reported previously. Westin et al.9) reported that quality of life was considerably affected following a cardiac event such as AMI or revascularization procedures, especially during the initial recovery phase. Importantly, residual impairment of quality of life persists in these subjects over 1-year follow-up despite substantial improvement over time. Xie et al.10) reported through the Medical Expenditure Panel Survey in a random sample of the United States non-institutionalized population that CAD could provoke a significant impairment in both HRQoL and health utility, particularly with respect to physical health and self-rating health. Patients' perceived quality of life could provide important prognostic information as well. Rumsfeld et al.23) measured preoperative quality of life in patients undergoing coronary artery bypass graft surgery, and found that low scores on the physical component summary of HRQoL significantly predicted 6-month mortality following the surgery. Quality of life in patients with ischemic heart disease was found to be a predictor for 10-year mortality.24) Therefore, our data suggested that treatment of patients with CAD should aim at improving HRQoL in addition to improving mortality given the prognostic value of quality of life.
The primary and secondary control strategies were determined as significant independent predictors of ACS after adjustment of age and gender in the present study. The ACS group tended to use primary control strategy more, while the control group tended to use secondary control strategy more. Therefore, adjusting one's thoughts, feelings, and goals to conform to current situation (secondary control), instead of favoring proactive attempts to change one's environment (primary control), may be protective against ACS. Using primary control strategy is frequently ineffective in dealing with uncontrollable situations. Therefore, those who rely on primary strategies are more likely to experience frustration and negative emotions. Additionally, the tendency of pursuing primary control strategies involves aggression and dominance25) that can subsequently increase the risk of CAD.26) Thus, enhancing reliance on secondary control strategies may be more protective against development of CVDs. However, this notion needs further prospective study to be clarified.
Contrary to previous studies,8)22)27) the present study did not show any significant difference between the ACS group and control group in levels of psychological maladjustment such as anxiety, hostility, and work stress. A large-scale community-based study showed that men reporting 2 or more anxiety symptoms out of 5 items had elevated risk of fatal CAD and sudden death.27) However, this study included only men, although anxiety disorders are more common among women. The large-scale epidemiological studies of anxiety disorders among CAD patients are still lacking.
Hostility is a major attribute of type A behavior pattern, and encompasses negative orientation toward interpersonal relationships including anger, cynicism, and mistrust.28) The results of longitudinal studies assessing the relationship between hostility and CAD in healthy subjects are mixed, with positive and negative results.28) There is no large scale epidemiological study assessing the role of hostility among CAD patients thus far.
Job strain, defined as jobs with high demand with low decision latitude, has emerged as an important risk factor for CVDs.28)29) In a recent review, in 7 of the 13 cohorts, high job strain is a significant risk factor for CVDs with risk estimates ranging from 1.33 to 2.62, but negative studies have also been reported.29)
Several factors could be postulated as a source of data discrepancy between ours and other positive studies. Firstly, difference in measures of psychological maladjustment might be a factor. Measurements used in other studies assessed different aspects of anxiety, hostility, and work stress based on different theoretical framework or construct. For example, there are several postulated models regarding to job stress model, such as the job strain model, the effort-reward imbalance model, and the organizational injustice model. Secondly, different time periods of assessing psychological states might be another factor. While other studies assessed psychological states quite early after admission to the hospital, the present study measured psychological states 2-3 weeks after onset. A study of trajectory of anxiety level in patients with AMI showed that the highest level of anxiety occurred within 12 hours after AMI, and that anxiety level decreased over time.30) Therefore, it is probable that our analysis might underestimate anxiety level in the ACS group during the early peak period.
Most of other studies have explored each psychological factor separately. The strength of the present study was that multiple psychological factors including psychological well-being, ill-being, and control strategy factors were examined simultaneously. The integrated approach of the present study enabled us to understand better the overall psychological status of ACS patients. Moreover, the present study identified a subset of ACS patients with psychological vulnerabilities that might be closely associated with ACS development. Although the need for assessing psychological states of CAD patients has been suggested in many studies, the measurement of psychological information is not yet practical. Based on our data, we can hypothesize that psychological factors such as low level of quality of life and proactive behaviors in achieving ones' goal (primary control) could be risk factors for ACS development. This hypothesis needs verification by further large-scale prospective studies.
The present study had several limitations. Firstly, there were substantial differences in gender, age, socioeconomic status, educational level, and marital status between the ACS group and control group. Statistical analysis was performed after adjusting age and gender. However, other factors associated with socioeconomic factors could also affect psychological status and development of ACS. Secondly, the subjects of the present study originated from a single institute and the number of subjects was not large. Thus extrapolating general trends from our data may have a limitation. Thirdly, detailed features of psychological status, such as age of first onset, diagnostics subtypes, number of episodes, and duration, were not included in assessments of psychological maladjustment. The magnitude of these detailed psychological features could vary over time, thus might affect the risk of ACS. Lastly, the present study had a cross-sectional design, therefore identifying a causative role of psychological factors in development of ACS is limited. Moreover, psychological evaluation was performed in the ACS group at around 2-3 weeks after ACS event, so data would reflect the acute state after ACS rather than steady state before ACS.
In conclusions, patients with ACS had poor HRQoL and had a tendency to be proactive in changing their environment rather than adjusting their thoughts, feelings, and goals to conform to the current situation. Our data did not show any significant impairment in anxiety, hostility, and job stress in ACS patients. Further large-scale prospective studies are needed to clarify the causative effect of comprehensive psychological factors on development of ACS.




 XML Download
XML Download