

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In ST segment elevation myocardial infarction (STEMI), simultaneous thrombosis formation in multiple coronary arteries is rare. Most patients with acute simultaneous total occlusion of more than two coronary arteries have poor prognosis. We report on a patient who presented with STEMI and was found to have simultaneous total occlusion of the distal portion of the coronary arteries. This patient was successfully treated with thrombus aspiration and systemic glycoprotein (GP) IIb/IIIa inhibitor.
Case
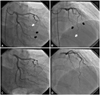
A 52-year-old male arrived at our emergency department with sustained chest pain and diaphoresis, starting 1 hour before presentation. He had no risk factors for coronary artery disease except that he was a male older than 45 years of age. On arrival, his blood pressure was 136/92 mm Hg and his heart rate was 90 beats/min. The initial 12 lead electrocardiogram showed a sinus rhythm with more than 2 mm ST segment elevation in the leads of I, II, aVF, and V3-V6 (Fig. 1). Sublingual nitroglycerin was not effective for relieving the chest pain. Emergency coronary angiography showed total occlusion of the distal left anterior descending artery (dLAD) and the second and third obtuse marginal branches (OM) of the left circumflex artery (Fig. 2A and B). The intravascular ultrasound (IVUS) revealed organized thrombus in the dLAD and there was no definitive critical atherosclerotic stenosis. The thrombus was removed with an export aspiration catheter (Medtronic, Minneapolis MN, USA) at dLAD. After thrombus aspiration, Thrombolysis in Myocardial Infarction (TIMI) 2 flow was obtained at dLAD and we decided to start the GP IIb/IIIa inhibitor. Neither balloon angioplasty nor stent implantation was done in dLAD because there was no critical atherosclerotic stenosis on IVUS. Although, the second and third OM showed TIMI 0 flow, we decided not to perform thrombus aspiration because the occlusions were located in the far distal portion of the OM, we had already started the GP IIb/IIIa inhibitor, and the patient was stable. He was continuously infused with intravenous GP IIb/IIIa inhibitor and heparin.
Ninety minutes after the procedure, the follow-up electrocardiogram showed improvement of ST segment elevations. Twenty-four hours later, the follow-up coronary angiogram showed TIMI3 blood flow at dLAD and second and third OM (Fig. 2C and D). After taking aspirin, clopidogrel, beta-blocker and statin, the patient was discharged 7 days later without complication.
Discussion
It is extremely rare in STEMI with simultaneous total occlusion of 2 or 3 coronary arteries, and it usually results in poor prognosis, including high mortality. Goldstein et al.1) demonstrated the presence of multiple unstable plaques and overlying thrombi in patients with acute myocardial infarction up to 32.8% and Burke and Virmani2) reported that 25-50% of patients who died of acute myocardial infarction had multiple coronary thromboses on autopsy. However, it is extremely rare for multiple coronary thromboses to be diagnosed in clinical practice because these patients tend to present with cardiogenic shock or a rapid and fatal course.3)
A possible mechanism of multiple coronary thromboses in acute coronary syndrome is the pan-coronary process of multiple coronary ruptures in different coronary arteries.4) Another possible mechanism is the first ischemic event causing impairment of blood flow to other vessels can lead to acute secondary thrombosis.3) In this case, although the IVUS study was not performed at the OM, the latter mechanism may give an account of our case because the left circumflex coronary artery and OM showed normal coronary angiography, except for distal occlusions of OM. The different reported cases of multiple coronary thromboses have been associated with aortic or mitral valve endocarditis, systemic thrombocytosis, and suspected coronary spasm.5)
Usually in cases of multiple coronary thromboses, patients present with cardigenic shock and an intra-aortic balloon pump needs to be inserted first before coronary intervention. In this case, the patient was relatively stable and the occlusions were located at the distal portion of the coronary arteries, which were occupied with thrombus except for critical atherosclerotic stenosis, and he was successfully treated with thrombus aspiration and GP IIb/IIIa inhibitor. There were some reports that thrombus aspiration drew better reperfusion in patients in STEMI,6)7) and that this strategy was pro-bably helpful in a subset of patients with thrombotic occlusion of the distal coronary artery without critical atherosclerotic stenosis. In addition, anti-platelet therapy with GP IIb/IIIa inhibitor and heparin, during and after intervention, is very useful in such cases to prevent further thrombus formation and to salvage the myocardium.

 XML Download
XML Download