

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
It is well known that arterial stiffness is increased by cardiovascular risk factors such as age, hypertension, diabetes, and chronic kidney disease. As a consequence of elevated arterial stiffness and decreased vascular distensibility, there is an increase in systolic blood pressure, which causes an increase in left ventricular workload and subsequent left ventricular hypertrophy, and a decrease in diastolic blood pressure, which leads to impaired coronary perfusion.1)2) There are various noninvasive methods for measuring arterial stiffness, such as ultrasound and MRI. These technologies detect changes in the diameter (or area) of an artery in response to distending pressure, and pulse wave velocity (PWV). Among these measurements, PWV is a simple index derived from pressure-sensitive transducers, doppler ultrasound, or applanation tonometry. Thus, it is widely used in clinical settings.3)4) PWV reflects the degree of arterial sclerosis, and aortic stiffness assessed by PWV is an independent risk factor for cardiovascular diseases.1)4)5) However, it is not known whether an increase in peripheral artery PWV is related to severity of coronary artery disease (CAD), or whether PWV can be used to predict CAD.
Invasive coronary angiography is the gold standard for detecting CAD. It is useful not only for the diagnosis of obstructive CAD, but also for determining the severity of CAD by evaluating the degree of luminal narrowing and identifying the anatomical location of the obstruction.6)
Coronary artery calcification develops as part of the atherosclerotic process, and therefore occurs almost exclusively in atherosclerotic arteries and is absent in normal vessel walls.7) Cardiac computed tomography (CT) is highly sensitive for detecting coronary artery calcium and is being used with increasing frequency to screen for CAD in both asymptomatic and symptomatic patients. Previous studies with cardiac CT reported that the severity of coronary atherosclerosis could be evaluated noninvasively, and that the prognosis of CAD could be predicted by coronary artery calcium scoring (CACS).7)8)
Brachial-ankle pulse wave velocity (baPWV) is the most widely used PWV index because of its convenience. The aim of this study was to evaluate the usefulness of baPWV as a predictor of the severity of coronary atherosclerosis. Furthermore, we assessed its value for predicting the severity and presence of obstructive CAD in high-risk patients suspected of having CAD.
Subjects and Methods
Study population
Between March 2005 and February 2008, 174 consecutive patients were enrolled, who had been referred for evaluation of suspected CAD and who had undergone both baPWV measurement and cardiac CT for CACS at the Seoul National University Bundang Hospital. Patients with a history of obstructive CAD were excluded. Based on clinical judgment, 92% of patients (160 of 174) underwent invasive coronary angiography.
Brachial-ankle pulse wave velocity
After a subject was in the supine position for 5 or more minutes, blood pressure and baPWV were measured using an automated waveform analyzer (Colin VP-2000, Colin Medical Instruments Corp., Komaki, Japan). Blood pressure was measured in both arms using the blood pressure cuffs of the device, and the higher value was used for further analysis. The mean of baPWV measured bilaterally was used for analysis.
Cardiac computed tomography
Scanning was performed using a 64-slice multi-detector CT scanner (Brillance 64; Philips Medical systems, Best, The Netherlands) with a tube voltage of 120 kV, tube current of 55 mAs, 200 mm, collimation of 40×0.625 mm, and gantry rotation speed of 0.40 second. The score for each calcified focus of coronary artery was determined by the method of Agatston et al.9) and the total value for CACS was obtained by summing individual focus scores from each of the 4 epicardial arteries (left main, left anterior descending, circumflex, and right coronary arteries).
Coronary angiography
Coronary angiography was performed at the discretion of the examining physician. The procedure was performed through the right radial artery, or, if that approach proved difficult, through the right femoral artery. Obstructive CAD was defined as coronary artery luminal narrowing greater than 50% by gross measurement. Moreover, if luminal narrowing greater than 50% involved the left main coronary artery or more than 3 coronary arteries, the patient was diagnosed with multi-vessel obstructive CAD.10) The severity of CAD was classified using the modified Gensini scoring system.6)
Statistical analysis
Values are expressed as means±standard deviation. Continuous variables were compared using the unpaired t-test, and categorical variables were compared using the χ2 test. Pearson product-moment correlation was used to assess the correlations between baPWV and CACS and modified Gensini scoring values. Multivariate logistic regression analysis was carried out to assess the odds ratios of baPWV for obstructive CAD. Receiver operating characteristic (ROC) curve analyses were used to determine the optimal baPWV cut-off values for predicting obstructive CAD. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 12 (SPSS Inc., Chicago, IL, USA), and p<0.05 was considered significant.
Results
Baseline clinical characteristics
The mean age was 63±9 years (n=174; range 33-92 years); 68% were male (118 patients), 74% were hypertensive (129 patients), 27% had diabetes (47 patients), and 49% had smoked within 3 months (86 patients).
Among 160 patients who underwent coronary angiography, obstructive CAD was detected in 130 patients (81%). Among them, 36 patients were diagnosed with multi-vessel obstructive CAD. The mean modified Gensini score of the 160 patients was 20.4±22.6. Patients with obstructive CAD had significantly higher values of total cholesterol (TC), low density lipoprotein cholesterol, C-reactive protein levels, CACSs, and modified Gensini scores compared with the patients without obstructive CAD, and there were no statistical differences observed in the other indicators (Table 1).
Correlation analysis of brachial-ankle pulse wave velocity and coronary artery calcium scoring
Among the entire study population, the baPWV significantly correlated with CACS by bivariate correlation analysis (r=0.25; p=0.001). However, after adjusting for factors influencing PWV, including sex, age, body mass index, blood pressure, heart rate, TC, and fasting blood sugar, baPWV no longer correlated with CACS (r=0.14; p=0.14) (Table 2).
Correlation between brachial-ankle pulse wave velocity and coronary artery disease severity
To evaluate the correlation between baPWV and CAD severity, simple correlation analysis was carried out between the baPWV and modified Gensini score. There was no significant correlation (r=0.10, p=0.19) seen, and also no significant correlation after adjustment for factors that influence baPWV (r=0.07, p=0.40) (Table 2).
The usefulness of brachial-ankle pulse wave velocity as a predictor of obstructive coronary artery disease
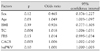
By multivariate logistic regression analysis, significant predictors of obstructive CAD were age, TC level, and CACS; whereas baPWV was not revealed to be predictive of obstructive CAD (Table 3). In order to assess the usefulness of baPWV as a predictor of obstructive CAD, we attempted to determine the optimal cut-off baPWV value by ROC curve analysis. The cut-off point 1,546 cm/s showed 53% sensitivity and 50% specificity in predicting obstructive CAD, and the cut-off point 1,593 cm/s showed 59% sensitivity and 55% specificity in predicting multi-vessel obstructive CAD (Fig. 1).
Discussion
Aging induces structural and functional changes in vessel walls. These changes include arterial wall hypertrophy, increased calcium deposition, and quantitative and qualitative changes in the collagen of the medial layer, which leads to disorganized microarchitecture. As a result, vessel wall compliance and elasticity decrease, and the PWV increases because of increased arterial stiffness.11) In addition, changes in blood vessel tension and elasticity caused by increased blood pressure also have an impact on measured PWV, along with gender, diabetes, renal failure, and salt intake.12)13)
Increase in arterial stiffness measured as increased PWV, has been reported to be associated with atherosclerosis and the CAD.5)14) Previous studies using aortic pulse wave velocity (aPWV) reported increases in odds ratio by 1.34 for cerebrovascular accident,15) 1.38 for CAD,5) and 1.23 for cardiovascular mortality,16) for each increase of aPWV by 340 cm/s. There are several mechanisms that might explain the association between increased PWV and CAD. Arterial stiffness causes premature return of the reflected pulse wave in late systole, leading to an increase in central pulse pressure and, consequently, to increased load on the ventricle. This results in decreased ejection fraction and increased myocardial oxygen demand.5) In addition, the decreased absorption capacity of the arterial wall leads to wall injury, which accelerates the progression of atherosclerosis.17)
This study also evaluated the usefulness of baPWV, the most widely-used PWV index, for prediction of obstructive CAD, and whether baPWV correlated with the severity of coronary artery calcification or CAD in high-risk patients. Although the CACS is a good reflection of the severity of coronary atherosclerosis and the prognosis of CAD, its value is limited for predicting the presence and severity of obstructive CAD.18) To compensate for the limitations of CACS, we evaluated the presence of obstructive CAD with modified Gensini scoring and invasive coronary angiography to identify CAD.
baPWV correlated neither with CACS nor with modified Gensini scoring after adjusting for factors influencing PWV. By multivariate logistic regression analysis, baPWV failed to predict obstructive CAD. In addition, baPWV showed low sensitivity and specificity for predicting the presence of obstructive CAD and multi-vessel obstructive CAD by ROC curve analyses.
Several studies have investigated the relationship between arterial stiffness and atherosclerotic burden. Megnien et al.19) reported that aPWV did not correlate with the degree of CACS, and that aPWV was mainly affected by aging and blood pressure, etc.; therefore aPWV could not predict coronary atherosclerosis in asymptomatic patients with risk factors for cardiovascular disease. But study results were inconsistent. Haydar et al.20) reported that aPWV was closely associated with CACS in patients with chronic kidney disease, and Kullo et al.14) showed similar results in 401 asymptomatic patients.
While most of the previous studies were performed in asymptomatic patients or in those at low risk for CAD, most of our study patients either had obstructive CAD or they were at high risk for CAD. Accordingly, our mean CACS (305.1±6.8) and baPWV (1,651±354 cm/s) were higher than those of other study populations. Tsuchiya et al.21) showed that a cut-off value of 1,800 cm/s for baPWV predicted CACS values greater than 100 with 70% sensitivity and 79% specificity in asymptomatic patients with diabetes. In our study, however, the same cut-off value predicted a CACS greater than 100 with only 29% sensitivity and 87% specificity. This result may demonstrate the wide variation among study populations.
Xu et al.22) reported on a study of 272 patients with documented CAD showing that baPWV and ankle-brachial index were useful in predicting CAD and peripheral artery disease, and that a baPWV greater than 1,800 cm/s was suggestive of severe atherosclerosis as well as obstructive CAD. In the current study, we applied the method of Xu, and divided the patients into 4 groups according to their modified Gensini score as follows: Gensini score=0, 0.01-3.00, 3.01-32.67, >32.68. There was a significant difference in baPWV between the highest and lowest modified Gensini score group (p=0.049) without adjustment for age. It is well known that increasing age is the most decisive factor for increasing PWV regardless of the presence of atherosclerosis.23) In our study, there was also a highly significant correlation between age and baPWV (r=0.57, p<0.001), and after adjusting for age, there was no significant correlation between baPWV either with CACS or with modified Gensini scoring. By multivariate logistic regression analysis that included age, baPWV was not revealed to be a predictor of obstructive CAD.
Marchand discovered that fatty degeneration was involved with arterial stiffening in 1904, and introduced the term "atherosclerosis". Although the increase in arterial stiffness and the progression of atherosis share the same pathophysiological factors, their association and causality are not well understood. Besides the progression of atherosclerosis, increased arterial stiffness is associated with vessel wall changes such as increase in collagen fibers, and decrease in elastin and vascular smooth muscle tone, in addition to "extrinsic factors" such as hormones, salt, and glucose.24) After excluding age, cholesterol plays an important role in the progression of atherosis, while blood pressure seems to play a more important role in the progression of arterial stiffness.25) Therefore the increase in PWV, which represents arterial wall stiffness, does not simultaneously increase to the same degree as progression of atherosis.
While previous studies have used aPWV, which represents central arterial wall stiffness, in this study we used baPWV, which has been increasingly used as an index of arterial stiffness because of its convenience. However, baPWV has some limitations. First, the pulse wave does not propagate directly from the brachial arteries to the posterior tibial arteries in the same arterial tree; thus, baPWV is indirectly estimated using the PWV from the heart to the brachial and posterior tibial arteries. Second, compared to the central arteries, peripheral arteries do not represent aging and disease-related changes as well.26) Although Sugawara et al.27) reported that baPWV provided similar qualitative information to information derived from central arterial stiffness, the best indicator reflecting central artery stiffness is considered to be aPWV measured as the carotid-femoral PWV.28)
Because of its convenience, the examination of peripheral artery stiffness is widely used in various patient groups with risk factors for CAD. Although some studies reported that patients at high risk for CAD can be screened using baPWV, the current study demonstrates that baPWV does not directly correlate with coronary artery calcification and severity of CAD in high-risk patients. Furthermore, baPWV also has low sensitivity and specificity for predicting obstructive CAD. Consequently, it may be of limited value as a screening tool for CAD in high-risk patient groups.
As mentioned previously, the current study population included 130 patients with obstructive CAD out of 160 patients who underwent coronary angiography. Our study population differed significantly from those in other studies. Therefore extrapolating the findings of our study to the general population is difficult, and further studies of various study populations are needed. Furthermore, since there is a significant difference between aPWV and baPWV, future studies evaluating arterial wall stiffness should include these different indices.


 XML Download
XML Download