

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Distal radius fractures are one of the most frequently treated upper limb injuries1) that are often associated with complications such as impaired mobility and stiffness of noninvolved finger joints mainly due to posttraumatic and post-immobilization edema of the hand.2345) Early initiation of joint motion and preservation of adjacent joint motion can be important to prevent finger stiffness after distal radius fractures and should be taken into consideration in selecting treatment and immobilization methods.67)
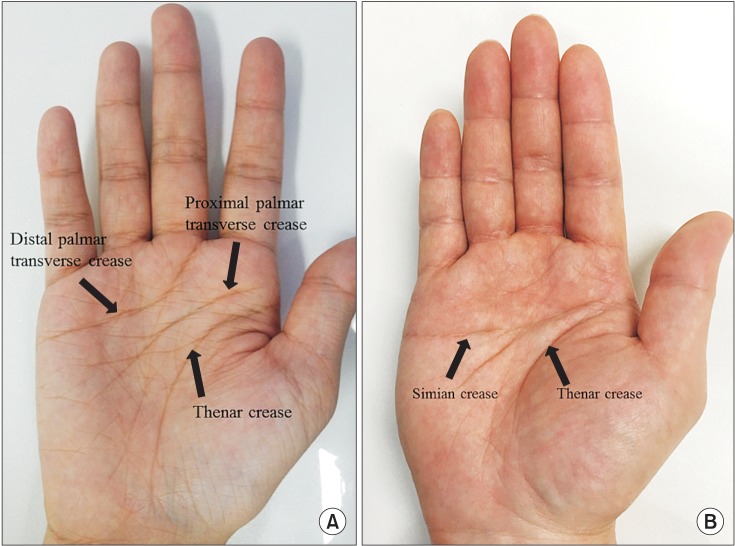
To the best of our knowledge, there are no detailed descriptions or established guidelines regarding proper location of immobilization devices at the distal end of the wrist for preservation of finger motion. In the meantime, the distal volar end of wrist immobilization has been commonly located just proximal to the midpalmar region or proximal to the metacarpophalangeal joint (MCPJ) in order not to limit MCPJ motion.8910) However, the definition of midpalmar region is vague and there are too diverse individual palmar crease patterns to use as a reference point during the application of a splint (Fig. 1). Therefore, it would be helpful to establish the proper physical and radiological locations of the distal end of wrist immobilization. In this study, we aimed to determine the suitable distal location of wrist immobilization with a short arm splint, the simplest form of wrist immobilization. Radiological evaluation is not mandatory to identify the distal location of a splint; however, it could give us additional information on whether the distal end of a splint is properly located.
We hypothesized that there would be a constant reference line for application of the volar short arm splint and radiological findings regarding the distal locations of the volar short arm splint would be informative. The goals of this study were to compare maximal MCPJ flexion angles after application of a volar short arm splint at three different locations and verify the relationship between the 3 different physical and radiological locations.
METHODS
Forty healthy volunteers (20 males and 20 females) with a median age of 31 years (range, 21 to 49 years) were recruited for the study. The exclusion criteria were patients with a history of trauma to the hand and wrist and ailments such as arthritis, flexor tenosynovitis, trigger finger, and Dupuytren's disease in the hand and wrist that could limit the range of motion of the fingers.
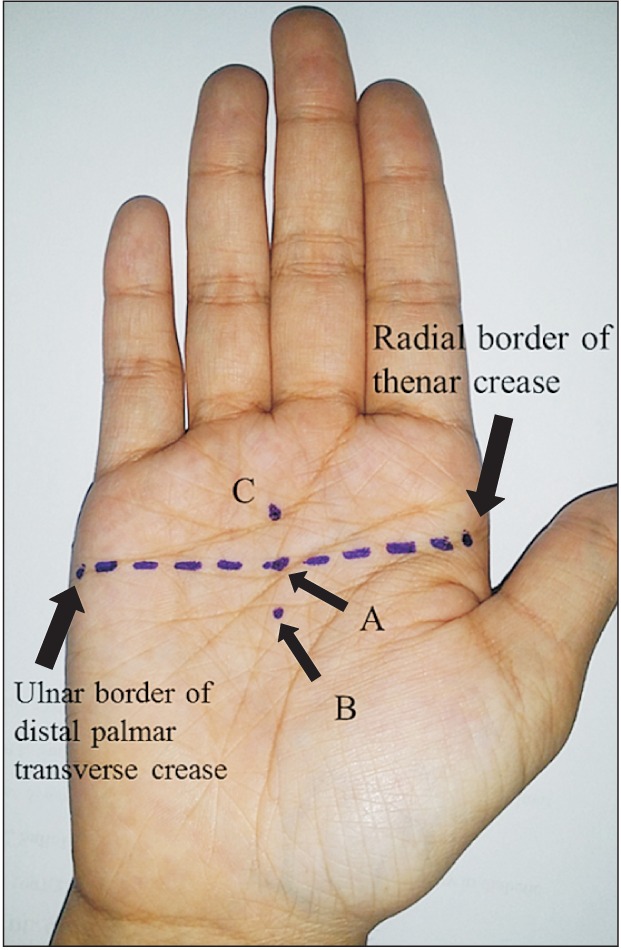
A transverse line that forms on the palm during MCPJ flexion between the radial end of the thenar crease and the ulnar end of the distal transverse palmar crease (transverse skin folding line) was drawn. Location A was designated at the center of this line that is usually located between the distal and proximal transverse palmar creases. Location B was determined at 1 cm proximal to location A. Location C was determined at 1 cm distal to location A, which is usually located between the distal transverse palmar crease and the proximal digital crease. We applied a volar short arm splint on the dominant hand of the study subjects at each location (Fig. 2).
The volar short arm splint was constructed to a size of 4 inch × 15 inch (10 cm × 38 cm). The distal end of the splint was cut to be parallel to the palmar digital crease of each patient and the distal center of the splint was applied to the 3 designated locations. A 4-inch (10-cm) elastic bandage was then applied over the splint to cover the splint completely and prevent movement of the splint.
Two orthopedic surgeons measured the MCPJ flexion angle using a manual goniometer. At first, maximal flexion angle of the MCPJ was measured at each finger without application of the splint as control. Measurements were repeated after application of the splint at each of the 3 locations; the subjects were instructed to flex their fingers until there was any resistance during flexion.
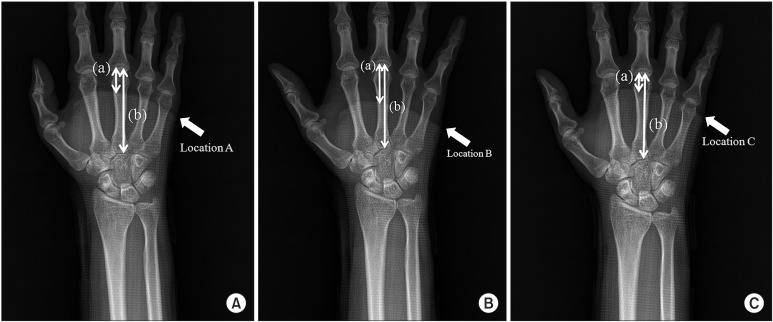
The locations of the distal end of the volar short arm splint were evaluated on anteroposterior radiographs of the wrist. The distance from the metacarpal head to the distal end of the splint was measured for every metacarpal bone of all subjects and the ratio to the whole metacarpal bone length was calculated in percentage (Fig. 3).
A sample size calculation was performed with an 80% power to detect a minimum difference of 5° in MCPJ flexion angle assuming a standard deviation of 10°. Although the minimum requirement was 33 patients, seven more patients were added to the cohort; therefore, a total of 40 subjects were enrolled in this study.
The Wilcoxon signed-rank test was used to compare the maximal flexion angle of the MCPJ and the radiographic location that was measured as the ratio of the distance between the metacarpal head and the distal end of the splint to the total metacarpal bone length. The interrater reliability of the measurements was evaluated with use of the intraclass correlation coefficient (ICC). A p-value of less than 0.05 was considered statistically significant. All statistical analyses were conducted with SPSS ver. 16 (SPSS Inc., Chicago, IL, USA).
RESULTS
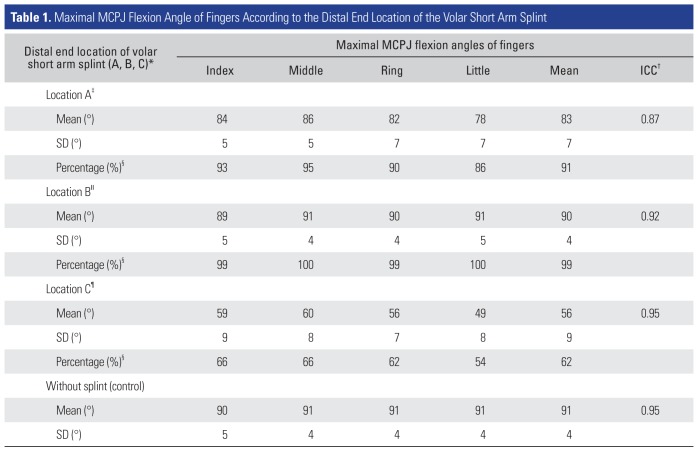
The maximal MCPJ flexion angles according to the 3 different distal locations of the volar short arm splint were measured by two observers who were orthopedic surgeons (Table 1). The ICC of the interrater reliability for the measurement of maximal MCPJ flexion angle at each location was over 0.80 (excellent agreement) in every measurement of the fingers. When the splint was applied at location A and C, the maximal MCPJ flexion angle decreased to a mean of 83° (91% of control value) and 56° (62% of control value), respectively (compared to the control, p < 0.001). At location B, the maximal MCPJ flexion angle was a mean of 90° (99% of control value); no significant difference was observed compared to the control (p = 0.103). There was also significant difference in the average maximal MCPJ flexion angles among location A, B, and C (location A vs. location B, location B vs. location C, and location A vs. C, all p < 0.001).
In the comparison of maximal MCPJ flexion angles among fingers, the maximal MCPJ flexion angles of the little finger at location A and C were significantly lower than those of index, middle, and ring fingers (p < 0.001) (Table 1).
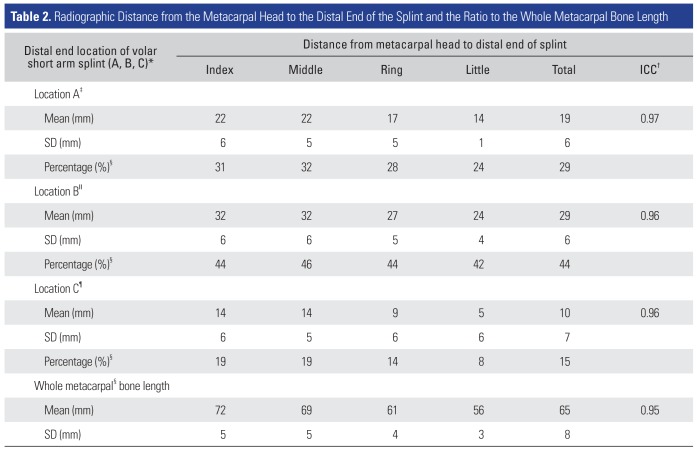
The results of radiological evaluation of the distance from the metacarpal head to the distal end of the splint at each finger are described in Table 2. The average length from the metacarpal head to the distal end of the splint at all fingers decreased in the order of location B, A, and C (29 mm, 19 mm, and 10 mm, respectively; p < 0.001). The average ratio of each location to the whole metacarpal bone length was 44% at location B, 29% at location A and 15% at location C (p < 0.001).
DISCUSSION
The current study demonstrated that the MCPJ flexion was limited to 91% of the control when the distal end of the volar short arm splint was located at the transverse skin folding line of the palm. The MCPJ flexion was well preserved when the distal end of the volar short arm splint was located at 1 cm proximal to the transverse skin folding line. Since the influence of 91% maximal MCPJ flexion angle compared to the control on finger stiffness has never been reported, we cannot confirm if the decrease is within an acceptable range. However, we believe that the ideal location of the distal end of the volar short arm splint for complete preservation of MCPJ flexion is more proximal to the transverse skin folding line, not on the transverse skin folding line.
At location A and C, the little finger was more limited in MCPJ flexion than other fingers. Therefore, we postulate that a splint with more removed design at the little finger would be preferable for maximal MCPJ flexion.
On the radiological evaluation, the average distance from the metacarpal head to the distal end of the volar short arm splint at location A and B was 19 mm and 29 mm, respectively. The average ratio of the distance to the whole metacarpal bone length was 29% at location A and 44% at location B. Based on these results, we suggest that the distal end of the volar short arm splint should be placed proximal to 29 mm (44%) from the metacarpal head to the whole length of metacarpal bone radiologically to preserve the MCPJ flexion angle perfectly.
Bugbee and Botte11) reported that anatomy textbooks and reports paid little attention to the relationships between skin creases of the hand and underlying anatomic structures; therefore, there is a lack of quantitative assessments of these relationships and a surprising lack of agreement in the descriptions provided. They also reported that a line joining the radial and ulnar borders of the transverse palmar creases usually marked the level of the metacarpal necks, not the MCPJs. In our study, location A was located at a line joining the radial border of the thenar crease and ulnar border of the transverse palmar crease and the radiological result supports the previous report that the transverse palmar crease corresponds to the metacarpal neck. However, the transverse palmar creases are of varying patterns depending on the individual as some people do not have a separated proximal and distal transverse palmar crease and instead have one transverse palmar crease that is called a simian crease. Therefore, we cannot establish the proximal transverse palmar crease or the distal palmar crease as a single reference line. The thenar crease also has a variable morphology and its vertical appearance might not be useful as a reference line for application of a volar short arm splint.
In order to determine the proper distal location of the volar short arm splint, we have to define a reference location for MCPJ flexion that is identifiable on the surface of the hand. In this respect, we recognize that the central part of the palmar and thenar creases is more variable and the peripheral part of them is likely to be more constant. A line joining the radial and ulnar borders of the transverse palmar creases or the radial border of the thenar crease and the ulnar border of the distal transverse palmar crease is the constant skin folding line of the MCPJ, which usually marks the level of the metacarpal neck. Therefore, we defined this line as transverse skin folding line and used it as a reference in this study. We believe it could be a useful anatomic landmark for similar surface anatomy and placement studies in the future.
There are some limitations in our study. First, MCPJ flexion angle measurements were performed in normal healthy subjects without any trauma; thus, there is a possibility of observing different results from subjects with hand or wrist injuries. Second, this is a time zero study and we do not know whether the restriction of MCPJ flexion by the volar short arm splint might affect MCPJ stiffness. Third, the resistance that restricted further flexion of the MCPJ is a subjective value that could be different among subjects. Finally, we need to assess the impact of distal location of the volar short arm splint on finger stiffness in the clinical setting and various locations should be examined for optimal placement of the volar short arm splint after distal radius fracture surgery.
In summary, we recommend that the distal end of the volar short arm splint should be located at minimum 1 cm proximal to the transverse skin folding line to preserve MCPJ motion perfectly, which is located at distal 44% of the whole metacarpal bone length on the radiograph.
 XML Download
XML Download